 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 65-66 Case Report Fungemia caused by Verticillium species in an immunocompromised child Bashir *G, Thokar MA, Ahmad S, Fomda BA, Lone R, Fazili T Department of Microbiology (GB, MAT, BAF, RL, TF) and Department of Medical Oncology (SA), Sher-i-Kashmir Institute of Medical Sciences, Soura-190 001, Jammu & Kashmir, India Correspondence Address: Bashir *G, E-mail:
drgulnazbashir@hotmail.com Code Number: mb06015 Abstract The incidence of fungal infections is increasing due to immunocompromised states. We report a case of fungaemia due to a rare fungus - Verticillium , in a 6 year old child diagnosed as a case of acute lymphoblastic leukaemia- L1 with high grade fever. The patient was treated with amphotericin B with a good clinical response.Keywords: Fungaemia, Verticillium, immunocompromised
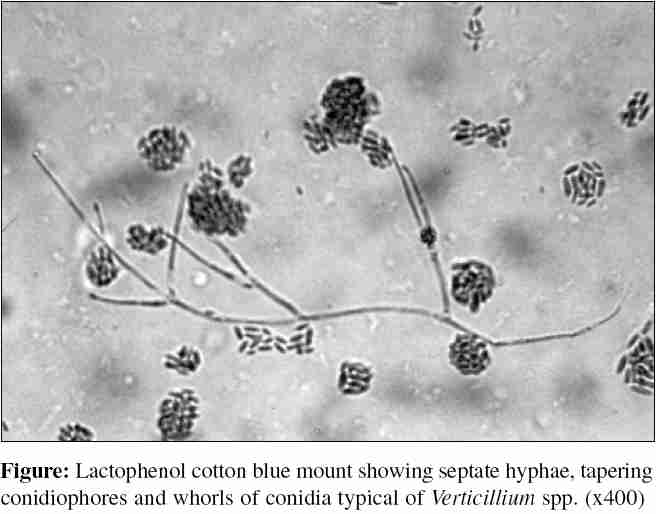
Systemic fungal infections have been on the rise during the last two decades. Rare fungi, such as Mucor , Fusarium , Paecilomyces are emerging as causes of systemic fungal infections in immunocompromised hosts.[1] We report a case of fungaemia caused by a rare fungus - Verticillium , secondary to an infected central venous line, in a 6 year old patient with acute lymphoblastic leukaemia - L1 treated with multiple courses of chemotherapy. Patient responded to systemic amphotericin B therapy following removal of the central line. Case Report Six year-old male child, diagnosed as a case of acute lymphoblastic leukaemia-L1 received first session of induction therapy in November 2003 in the form of cyclophosphamide, cytarabine, methotrexate and 6-mercaptopurine with uneventful induction and postchemotherapy periods. Second session of induction therapy was started on 5th January, 2004. The patient developed fever on tenth day of induction therapy with a temperature range of 100-102°F and physical examination revealed pallor without any focus of infection. Investigative profile revealed haemoglobin 6.5 mg/dL; total leucocyte count 2.85x103/mm 3; differential leucocyte count: neutrophils 89%, lymphocytes 6%; platelets 38,000/mm 3sub , and absolute neutrophil count 2550/mm 3. Blood, urine and cerebrospinal fluid cultures were sterile after 48 hours of aerobic incubation. Patient was administered inj. cefepime 500mg i/v b.i.d and amikacin 200mg i/v b.i.d but continued to be febrile. Repeat blood culture on 13th and 14th day of induction from two different venepuncture sites revealed growth of a mould after 48 hours of aerobic incubation from routine blood culture bottles. Colonies on routine bacteriological media viz; blood and MacConkey agars were buff coloured and velvety after 48 hours of aerobic incubation at 37°C. Lactophenol cotton blue preparation of the mould revealed hyaline septate hyphae with erect, septate conidiophores showing tapered branching. Tips of the branches yielded conidia in the form of whorls [Figure - 1]. All the features of this mould were suggestive of Verticillium spp. [2] Central venous line was removed and its tip was cultured which revealed the same fungal species after 48 hours of aerobic incubation at 37°C. Antifungal treatment in the form of amphotericin B (0.15 mg/kg) was added to the treatment regime and the patient became afebrile after 48 hours. Treatment was continued for 10 days after which the patient remained afebrile and was discharged to follow up in the out patient department of medical oncology. Discussion Verticillium is a rapidly growing hyaline septate mould which rarely causes infection in humans. It causes infections mainly in immunocompromised hosts. There are reports of Verticillium keratitis,[3] subcutaneous infection[4] and peritonitis.[5] Our patient, who was immunocompromised due to the disease and chemotherapy with a TLC of 2.85x103/mm 3, was treated with broad spectrum antibiotics for high grade fever without any response. Initial cultures were sterile. A repeat septic screen revealed fungaemia due to Verticillium spp. on two occasions. As the same fungus was isolated from the central line tip, possibly the patient had contracted the infection through colonized central line. Infections due to Verticillium have responded to various antifungal agents including polyenes and azoles.[3],[4],[5] As these infections are rare there are no clinical therapeutic trials and hence no standardized guidelines for treatment are available. Hence, successful outcome requires early diagnosis, removal of an infected focus and selection of appropriate antifungal therapy based on microbiological identification of the fungus. Infection in our patient was diagnosed early, the infected central venous line was removed promptly and he was started on systemic amphotericin B with a good clinical outcome. Unfamiliar fungal isolates are frequently mistaken for environmental contaminants. In all immunocompromised patients presenting with fever, growth of rare fungi should be considered in the differential diagnosis of fungaemia if the same fungus is isolated from blood drawn from different venepuncture sites. To the best of our knowledge, this is the first report of fungaemia due to Verticillium spp. in a patient of acute lymphoblastic leukaemia on chemotherapy. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06015f1.jpg] |
| |||||||||
{kind=link}