 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 67-69 Case Report A case of human thelaziasis from Himachal Pradesh Sharma *A, Pandey M, Sharma V, Kanga A, Gupta ML Department of Microbiology, Indira Gandhi Medical College and Hospital, Shimla - 171 002, Himachal Pradesh, India Correspondence Address: Sharma *A, E-mail: dr_anu03@yahoo.co.in Code Number: mb06016 Abstract Small, chalky-white, threadlike, motile worms were isolated from the conjunctival sac of a 32 year-old woman residing in the Himalaya mountains. They were identified as both male and female worms of Thelazia callipaeda . To the best of our knowledge, this is the second case report of human thelaziasis from India.Keywords: Human thelaziasis, Oriental eyeworm
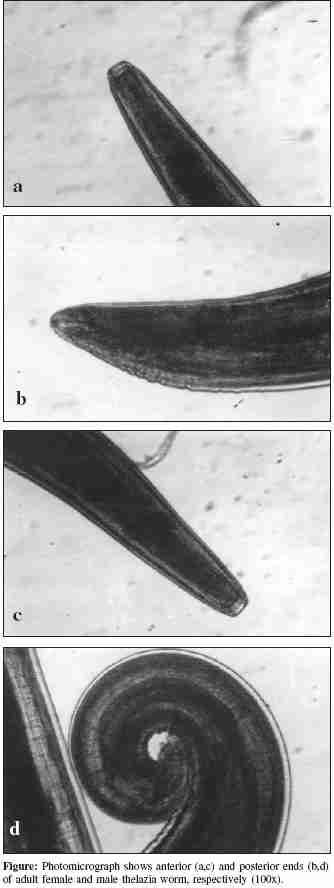
Thelazia callipaeda was first reported by Railliet and Henry in 1910 from a Chinese dog and it is also known as Oriental eyeworm. The first human case was reported by Stucky in 1917 , who extracted four worms from the eye of a coolie in Peiping, China . Since then a number of species of eyeworm have been reported in certain animals and birds from different countries of the world.[1] The two important species infecting human eye are Thelazia callipaeda and, rarely, Thelazia californiensis . T. callipaeda is found in China, India, Thailand, Korea, Japan and Russia. Recently it has been reported from Northern Europe and Southern Italy. Whereas, T.californiensis occurs exclusively in Western United States.[2],[3] In Asia, this spiruroid nematode is seen in the conjunctival sac, lacrimal gland and lacrimal duct of dogs, cats, cows, rabbits, badgers, deers, foxes and monkeys.[4] Man is an accidental host. Transmission occurs through face flies. Several species of the genera Amiota and Musca autumnalis (pest of livestocks) act as intermediate hosts. They ingest embryonated eggs when they feed on eye/nasal secretions of a sleeping host. Larvae develop in the body cavity of the fly and are deposited on the conjunctiva of a new host. The larvae take 3-6 weeks to reach maturity. Female worm lays eggs in the conjunctival and lacrimal sac of the host.[2] The most common clinical presentations are mild conjunctival irritation, foreign body sensation, excessive lacrimation, follicular hypertrophy and less often hypersensitivity to light, ocular pain, corneal opacities and ectropion.[1],[2] Secondary bacterial infections can worsen the symptoms, but the worms are generally not very pathogenic.[5] Nearly 250 cases of T.callipaeda infestation in humans have been reported worldwide.[2] Only two cases have been reported from India.[6] Case Report During autumn of 2004 a 32 year old woman from a rural mountainous region presented with the complaint of small, white, threadlike worms in her right eye. She was suffering with foreign body sensation and itching in her right eye for a few days. On looking in the mirror, she noticed moving worms in her eye. She could remove three worms with the help of a cotton wick. On her visit to the hospital, on examination, no worms were seen in the conjunctival sac. Conjunctiva was mildly congested. Patient was prescribed decongestant and was asked to report after one week. The patient belonged to a family rearing livestock and had a pet dog. On her second visit, thorough and careful examination of her eye revealed five worms coiled together in the upper fornix. They were removed with the help of forceps after instilling 4% lignocaine. The worms were motile and were sent to microbiology laboratory for identification. They were identified as T.callipaeda , there were two male and three female worms. Adult male worms measured up to 0.75 x 13.00 mm and female worms measured 0.85 x 17.00 mm. Transverse cuticular striations covered whole surface of the worm [Figure - 1]. The number of transverse cuticular striations at esophageal level, midportion and tail end helped in differentiating the two species ( T. callipaeda and T. californiensis ) and also male from female. Microscopically the buccal cavity was trapezoid, located anteriorly with no lips or teeth-like structures [Figure - 1] a,c. Males were ventrally curved, there were nine pairs of preanal and three pairs of postanal papillae, in [Figure - 1] d all of the preanal papillae were not seen because of the spiral coiling of the tail. In females, vaginal opening was anterior to oesophagointestinal junction and numerous, disc shaped encysted larvae lying in a row were seen in the distal uterus. In the posterior half of the body, unembryonated eggs filled the uterus.[2],[7],[8] The patient's all routine investigations including total leucocyte count, differentiated leucocyte count and peripheral smears were within normal limits. Removal of worms was sufficient to ameliorate the symptoms and there was no recurrence. Discussion Friedmann reported cases of Human Thelaziasis from India in 1948.[1] Singh et al reported two cases in 1993 from Manipur, which is a hilly state.[6] In this case report patient belongs to remote areas of Himalayan region. In other cases reported from China and Korea, a correlation with visiting the mountainous region has been seen.[1],[7] Our patient probably acquired infection from the livestock or the dog. There may have occurred many unreported cases, since extraction of the worm from the eye is all the treatment required. Clinicians should be made aware of the existence of this infestation as repeated migration of worms across the conjunctiva can result in scarification and fibrous opacity of the cornea.[1] The presence of white, threadlike, coiled masses in the conjunctival sac or migrating worm over the cornea are suggestive. Eggs and larvae can be seen in tears or eye secretions microscopically. Presence of embryonated eggs and fourth stage larvae in the conjunctival sac during the different parts of the year indicate seasonality in the reproductive activity of T.callipaeda , coinciding with the presence of vector from early spring to early autumn.[3] Though, symptoms resolve immediately after the removal of the worms, irrigation with lugol's iodine or 2-3% boric acid can be used to remove worms from the lacrimal duct. Levamisole and ivermectin have shown to cure similar infestations in Asia and Europe. There is no vaccine for thelaziasis. Public health and prevention strategies are important in India, where high infestation rate is found among dogs.[2] References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06016f1.jpg] |
| |||||||||
{kind=link}