 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 1, January-March, 2006, pp. 72-74 Case Report A rare case of human trypanosomiasis caused by Trypanosoma evansi Powar *RM, Shegokar VR, Joshi PP, Dani VS, Tankhiwale NS, Truc P, Jannin J, Bhargava A Department of Microbiology(RMP, VRS, NST, AB), and Department of Medicine(PPJ, VSD), Government Medical College, Nagpur – 440 003, Maharashtra, India; Institute de Recherche pour le Developpment (PT), Unite de Recherche 117 Trypanosomoses africaines, Montpellier, France and Communicable Disease Control, Prevention and Eradication (JJ), WHO, Geneva, Switzerland. Department of Microbiology, Government Medical College, Nagpur - 440 003, Maharashtra Correspondence Address: Powar *RM,
rajarampowar1@yahoo.co.in Code Number: mb06018 Abstract Human trypanosoma infections like the ones seen in Africa and South America are unknown in India. The only exception in literature is of two documented cases of a self-limiting febrile illness, being attributed to Trypanosoma lewisi like parasites. We are reporting an unusual case of trypanosomiasis from the rural parts of Chandrapur district in Maharashtra. An adult male farmhand who used to practice veterinary medicine also, presented with history of febrile episodes on and off since five months and drowsiness before admission to this Institute. Though routine blood and other investigations were within normal limits, the peripheral smear showed a large number of trypanosomes which morphologically resembled the species Trypanosoma evansi , the aetiological agent of surra - a form of animal trypanosomiasis. A battery of assays covering the spectrum of parasitology, serology, and molecular biology confirmed the infecting parasite to be T. evansi . Failure to demonstrate the central nervous system (CNS) involvement, as evidenced by the absence of parasite in cerebrospinal fluid (CSF) advocated the use of suramin - the drug of choice in early stage African trypanosomiasis without any CNS involvement. Suramin achieved cure in our patient. The case is being reported because of its unique nature as the patient was not immunocompromised and showed infestation with a parasite which normally does not affect human beings.Keywords: Trypanosomiasis, Trypanosoma evansi
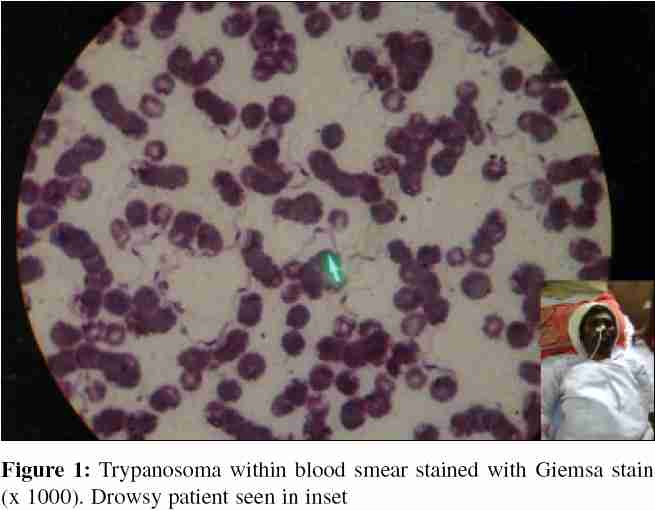
Human trypanosomiasis is unknown in India but is endemic in Africa and South America. This vector borne disease[1] known as sleeping sickness in Africa is transmitted by the infected saliva of tsetse fly during its blood meal and its South American counterpart, known as Chagas' disease is transmitted mechanically through infected faecal matter of Reduviid bug. African trypanosomiasis (Gambian, Rhodesian and Zambesi form of sleeping sickness) is caused by the human strain of Trypanosoma brucei whereas, South American trypanosomiasis (Chagas' disease) is caused by Trypanosoma cruzi . The third trypanosome which infects human beings is Trypanosoma rangeli . It is nonpathogenic and is isolated from human blood in Venezuela and Colombia. Apart from these human trypanosomes, various animal trypanosomes are also known which may be non pathogenic or pathogenic. T. lewisi is the non pathogenic trypanosome found in rats and transmitted by rat flea. The pathogenic trypanosomes include T. brucei (animal strain) found in tropical Africa and Transmitted by G morsetans causing nagana in domestic animals, T. evansi transmitted mechanically by tabanid and causing surra in horses and mules in India, T. equiperdum transmitted venereally in horses and asses in Europe, America, North Africa and India, T. equinum found in South America is transmitted mechanically by tabanid and causes mal de caderas in horses and T. vivax and T congolense transmitted by tsetse fly and causing disease in cattle. Trypanosomes of animals usually do not cause human infections. Rare instances of human infections due to trypanosomes found in animals are self limiting. [2] The present case had presented with a history of intermittent febrile episodes of five month duration which subsequently progressed to sensory deficit. Blood examination revealed intermittent parasitaemia with T. evansi , an animal trypanosome. With no evidence of immunosuppression, a serious, progressive infection by an animal trypanosome merits attention and is being reported here. Case Report A 46 year old male farmhand, resident of village Seoni in Sindewahi taluka of district Chandrapur from the state of Maharashtra reported to the casualty of Government Medical College and Hospital, Nagpur on September, 26th, 2004. He was admitted with a history of moderate grade fever since last 18 days and an altered sensorium since last 10 days. There was no history of vomiting and convulsions. Past history revealed that he had recurrent febrile episodes for the last five months. Personal history revealed that the patient was an unqualified veterinary practitioner. On examination, he was drowsy [Figure - 1] inset and responding sluggishly to oral commands. Patient was mildly febrile with a pulse rate of 88/minute and a correspondingly normal respiration rate. Blood pressure was recorded at 120/70 mm of Hg. and a small axillary lymph node was palpable on the right side. Systemic examination revealed that he had no neck stiffness or focal neurological deficit, spleen was just palpable cardiovascular system and respiratory system examination did not reveal any abnormality. A provisional diagnosis of cerebral malaria was made and peripheral blood smears were prepared and stained with Leishman stain. The red blood cells were normocytic normochromic, white blood cell count was within normal limits and platelets were adequate. However, the peripheral smear showed numerous trypanosomes, 20-25 ìm in size with the typical trypomastigote morphology of central nucleus, subterminal kinetoplast and a long flagellum with an undulating membrane. There was no evidence of malarial parasites. The findings of Leishman stained peripheral blood smear were further confirmed by staining peripheral blood smears with Giemsa stain [Figure - 1], Fildes' stain and JSB stain. Subsequent detailed investigations revealed his haemogram to be within normal limits. Bone marrow and cerebrospinal fluid samples did not reveal any parasites. HRP II for P. falciparum tested positive. Serum immunoglobulin estimation revealed the levels to be 2262 mg/dL for IgG, 60 mgs/dL forIgA and 256.25 mgs/dL for IgM. Test for HIV antibodies by ELISA was negative. The smear positive blood samples were inoculated intraperitoneally into a mouse, rat and guinea pig. Guinea pig and rat died after four days. Autopsy conducted on all three animals did not show any parasitaemia or changes suggestive of trypanosomiasis. Histopathology showed severe congestion and deposition of haemosiderin in liver and spleen. Parasite culture was attempted on Tobies medium procured from National Institute of Communicable Diseases, New Delhi. It turned out to be negative even after one month incubation. A card agglutination test for Trypanosomiasis (CATT) / T. evansi[3] (Institute of tropical medicine, Antwerp, Belgium) was done using whole blood and serum in the laboratory of Department of Microbiology, Govt. Medical College, Nagpur. This highly specific agglutination test was strongly positive for T. evansi (+++) and weakly positive for T. gambiense (++). Polymerase chain reaction (PCR) assays were done at the Institute de Recherche pour le D'evelopement in Montpellier, France using the collected blood samples to confirm the infection with T. evansi . DNA extraction was done using the mixed solution of blood or CSF equal volume with guanidine lysis buffer. A traditional phenol/chloroform/isoamyl extraction was performed. DNA templates (dilutions 1/100 and 1/1000) were kept at 4 0 C before use. Such dilutions were required to avoid inhibition due either to some remaining guanidine lysis buffer or a high concentration of DNA. Three PCR assays were performed using DNA trypanosomes from blood: a seminested PCR based on internal transcribed spacer (ITS) of rDNA, using primer ITS1/2 derived from KIN1/2 Primer[4] [Figure - 2]. This test allows the identification of the subgenus Trypanozoon. The second was a traditional single PCR of the 177 bp repeats for characterization of T. brucei group.[5] The third PCR assay was a T. evansi specific amplification using a 994 bp mitochordrial kinetoplast minicircle template and primers TEV 1/2.[6] Two reference strains were used. T. b. gambiense Bat 61 18 and T. evansi [Figure - 3]. The patient was initially treated with antimalarials. His fever subsided and the level of consciousness improved. However he again developed fever with demonstrable parasitaemia on 4th October 2004, 18th October 2004 and 21st November 2004. Gradually, the parasitic load decreased and stout and stumpy forms were seen in the peripheral smear. Subsequently on confirmation of T. evansi infection, he was treated with Suramin provided by WHO as Suramin is effective in T. evansi infection in cattle [7] and early stage African trypanosomiasis without any CNS involvement. Suramin was administered in a dose of 1 gm IV weekly for five weeks. After treatment the parasites disappeared from the blood and the patient's general condition improved. Discussion Africa and South America serve as endemic zones for human trypanosomiasis and in other geographical regions trypanosoma is confined strictly to animals. T. evansi is a strict animal pathogen causing surra in them. This case is first of its kind reported in medical literature. A wide spectrum of diagnostic tools involving parasitology, immunology and molecular diagnositc techniques were utilised to confirm the identity of the parasite beyond doubt. No CNS involvement was observed and the response of the patient to T. evansi specific drug Suramin was along the expected lines The mode of transmission of T. evansi in this patient remains unconfirmed. He had scars of injury on the palmer aspect of his right hand. A direct contact of the injured part with the infected blood or blood products from the cattle seems to be the most plausible route. Advent of HIV infection has led to many low-grade pathogens finding their place very frequently in medical literature. This case turned out to be HIV negative and that made his condition all the more intriguing. A purely animal pathogen infecting a normal human, causing clinical manifestations and responding very well to specific therapy makes this case first of its kind. Previous reports of isolation of trypanosoma resembling T. lewisi from the peripheral blood of two patients had mentioned a self limiting illness. Here, however, the patient harbored the parasites for close to five months and developed a full-blown clinical picture. Our case should increase awareness among physicians to include this condition in the differential diagnosis of pyrexia of unknown origin. Acknowledgement We thank Professor P Buscher (Institute of Tropical Medicine, Antwerp Belgium) and Professor E Delaporte (Institut de Recherche pour le Development, Montpellier France) for their kind help. We warmly thank Dr M Barrelt (University of Glasgow, Glasgow, United Kingdom) for his critical reading of the manuscript. Financial support: This work was supported by the Directorate of Health Services, Maharashtra State, India, the World Health Organization, and the Institute de Recherche pour le Development, France. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06018f1.jpg] [mb06018f3.jpg] [mb06018f2.jpg] |
| |||||||||
{kind=link}