 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
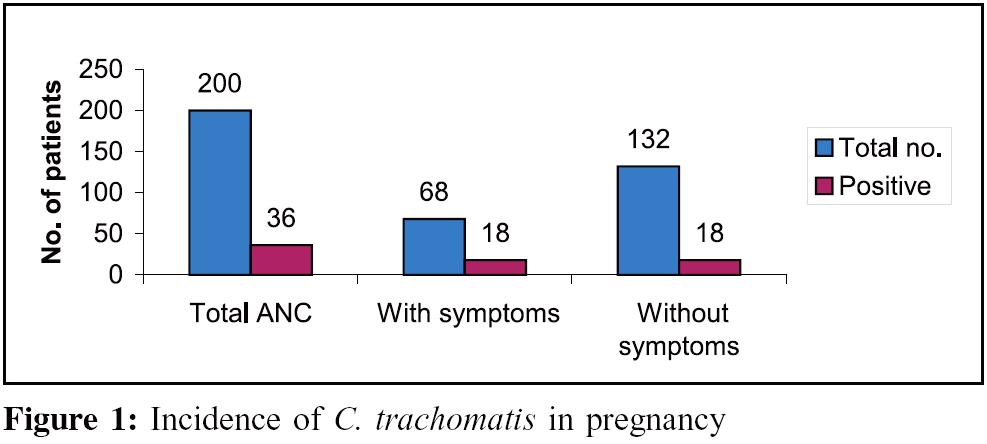
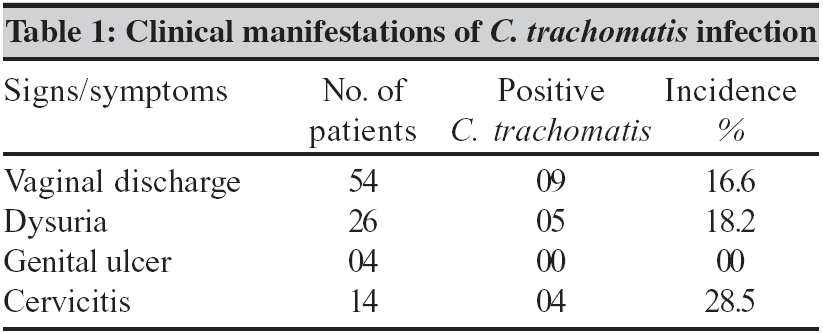
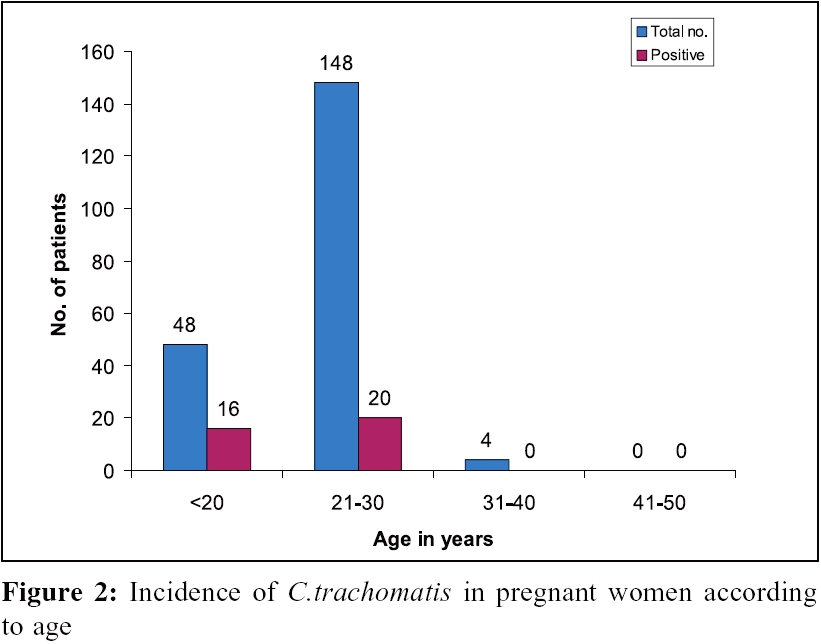
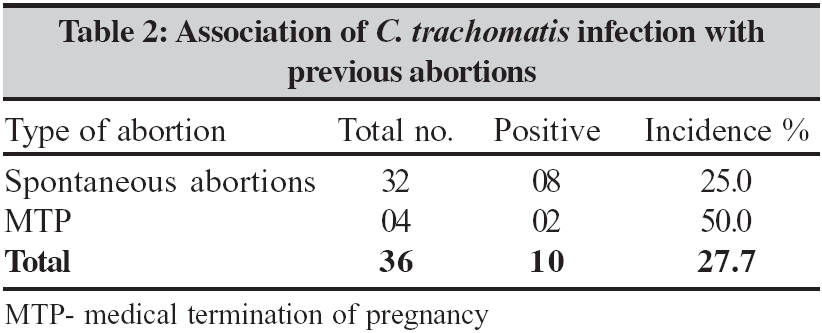
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 97-100 Original Article Chlamydia trachomatis antigen detection in pregnancy and its verification by antibody blocking assay *Malenie R, Joshi PJ, Mathur MD Department of Microbiology, Subharati Medical College, Meerut - 250 002. UP Code Number: mb06029 Abstract Purpose: To detect the prevalence of genital infection caused by Chlamydia trachomatis in pregnant women and also to confirm the positive results using blocking antibody assay.Methods: Endocervical specimens were collected from 200 symptomatic and asymptomatic pregnant women attending the ANC OPD at M P Shah Medical College, Jamnagar. The samples were tested for presence of Chlamydia trachomatis antigen using the monoclonal antibody. Blocking antibody assay was used to further verify the positive results. Results: Out of 200 pregnant women, 38 (19%) were found positive for Chlamydia trachomatis antigen. Out of the 68 symptomatic patients, C. trachomatis antigen was detected in 26.4%. After verification of the positive samples 13.6% of the asymptomatic pregnant women were found to be harbouring the infection in their genital tract. Two (5.2%) out of the 38 positive samples, on verification with the blocking antibody assay, were found to be false positive by IDEIA,TM thus the specificity of the IDEIATM being 94.8%. In patients with previous history of abortions, 27.7% were tested positive for C. trachomatis infection. Conclusions: Significant number of pregnant women shad C. trachomatis antigen in their endocervical canal, which can be easily diagnosed by this simple enzyme immuno assay having a specificity of 94.8%. Verification of positive results by antibody blocking assay can further improve the specificity of this non-culture test. Asymptomatic patients should also be screened for the infection. History of previous abortions places the patient at a higher risk for C. trachomatis infection thus such patients should be definitely tested for chlamydia infection. Keywords: Chlamydia trachomatis, antigen, blocking antibody, pregnancy C. trachomatis infection, a prevalent sexually transmitted disease, is associated with complications like ectopic pregnancy, fallopian tube block and adverse pregnancy outcome.[1],[2],[3],[4] In majority of the women the infection with this organism is asymptomatic or with minimal symptoms. Therefore, screening of women at risk is highly recommended. Women at highest risk often have the least access to health care facilities. Therefore there is a need for a rapid, simple and accurate test to detect C. trachomatis infection, which can be performed outside the laboratory setting when the patient is still in the clinical setting. Detection of C. trachomatis infection by non-culture techniques became feasible with the recent development of immunologic reagents specific for chlamydia. The direct fluorescent antibody (DFA) staining and enzyme immunoassay (EIA) are two such tests. C. trachomatis is an infectious agent in pregnant women. Depending upon the population studied and the method used for diagnosis the prevalence ranges from 2-37%[5],[6] Studies have proved a definite role of C. trachomatis infection in adverse pregnancy outcome.[1],[2],[3],[4] If not treated on time their newborns run a 20-40% risk of developing chlamydial conjunctivitis[7],[8],[9] and a 10-20% risk of developing chlamydial pneumonia.[7],[9],[10] Studies from India have reported that 15% of young asymptomatic women are positive for this infection.[11] In this study, an effort was made to detect C. trachomatis antigen from the endocervical specimens of the pregnant women and to verify the positive results with the antibody blocking assay so as to achieve the most accurate results. Materials and Methods Patients Clinical specimen Materials and Methods IDEIA™PCE Chlamydia and IDEIA™ Chlamydia blocking reagent manufactured by DAKO Diagnostics Ltd. Cambridgeshire, UK were used. Former is an immunoassay using dual amplification technology for detection of chlamydia antigen in endocervical swabs and the latter is a blocking antibody reagent, which is to be used in conjunction for verification of positive reactions. The IDEIA™PCE Chlamydia blocking reagents consist of two reagents: a genus specific murine monoclonal antibody (blocking reagent) of different origin to that used in the IDEIA™PCE Chlamydia test and a murine monoclonal antibody with no anti-chlamydial activity (control reagent). The selective blocking test is performed on specimens found to be reactive in the IDEIA™PCE Chlamydia test. Each reactive specimen is retested using two wells in the IDEIA™PCE Chlamydia test. If Chlamydia LPS antigen is present in the specimen, the blocking antibody (but not the control antibody), will selectively bind to it and block the binding of Chlamydial LPS to the capture antibody on the coated well. On completion of the IDEIA™ PCE Chlamydia test procedure, a significant reduction in the absorbance value obtained in wells containing the specimen or positive control and blocking reagent, relative to the wells containing the specimen or positive control and control reagent verifies the presence of chlamydia LPS antigen. Adding 0.05 to the mean of the negative control values calculates the cut off value. Statistical analysis Results Out of a total of 200 pregnant women included in the study group, 38 (19%) were positive for Chlamydia antigen. Sixty-eight patients had discharge per vagina, dysuria, genital ulcer and cervicitis, out of which 18 (26.4%) were positive for Chlamydia antigen [Figure - 1]. Cervicitis was the commonest finding [Table - 1] associated with C .trachomatis infection (28.5%). Among the 132 asymptomatic pregnant women 20 (15.1%) were positive for Chlamydia antigen [Figure - 1]. Out of the 20 asymptomatic women 18 (13.6%) were confirmed as positive with the blocking antibody assay while 2 (5.2%) were found to be false positive. The highest incidence (33.3%) of infection was found in the youngest of age group i.e, less than 20 years of age [Figure - 2]. History of previous abortions was present in 36 patients 32 of whom had spontaneous abortions and four underwent medical termination of pregnancy (MTP). Out of the patients with previous spontaneous abortion 27.7% were positive for Chlamydia infection, while 50% of patients with previous MTP were positive [Table - 2]. The 38 positive samples, which were positive with IDEIA, were re-confirmed by blocking antibody assay. Two (5.2%) were found to be false positive thus the prevalence of Chlamydia infection in pregnancy in our study group was 18%. All the discrepant results were from the asymptomatic group of pregnant women. Therefore, 13.6% of the asymptomatic group had chlamydial infection. The specificity of the EIA was 94.8%. Discussion Various authors using different techniques have reported the incidence of 6-37% Chlamydia infection in pregnancy.[3],[11],[12],[13],[14],[15],[16] An overall high incidence of Chlamydia antigen was detected in this study from the endocervical specimens, which was due to the study group selected. The study group comprised of patients of younger age belonging to poor socioeconomic group and included mostly the migratory population. Their partners were truck drivers/factory workers and defence personnel, thus placing their women at a higher risk of sexually transmitted diseases. Some reports of false positive Chlamydia antigen results could be because the patients who received pretreatment with antibiotics will remain asymptomatic although the antigen from the non viable Chlamydia can still be detected by EIA,[15],[18],[19] while cultures are positive only if the organism is viable. Therefore, authors who used the cell culture technique to isolate Chlamydia from the endocervical specimen reported a low incidence.[3] Quality of endocervical specimens collected can affect the incidence of false positive results because of its likely contamination with vaginal secretions.[20] EIA has been reported to give false positive results in presence of gram positive bacteria including Staphylococcus aureus, Streptococcus agalactiae, Peptostreptococcus spp. and gram negative organisms including N. gonorrhoea. Acinetobacter spp ,, Salmonella spp, E.coli and Gardenerella vaginalis. Kellogg and colleagues[21] tested Chlamydiazyme and the blocking antibody reagent with clinical isolates of bacteria and yeasts and found that the blocking of antibody eliminated the false positive results due to large concentration of some strains of gram negative bacteria. Much higher incidence (37%, 25.8%) was reported in a study group, which comprised of high-risk population.[13],[15] Low incidence (13.2%) reported by Grossman[16] from a high risk population of pregnant women is reported to be due to the increased transportation time (4 days) that was taken before the samples were processed and this had led to a loss of infectious particles/antigens. The sensitivity of EIA procedure has been reported to range from 44.4 to 100% for cervical specimens. The sensitivity of the C. trachomatis antigen assay is directly related to the number of Chlamydia present in the specimen. Asymptomatic carriage of 13.6% reported by us is a cause of concern. Although most infected women were asymptomatic, it has been reported earlier that at least half of infected people are carriers.[17] The age of peak incidence is late teens and early twenties, which is sexually the most active age. Genital infections caused by Chlamydia have been documented to be associated with abortions, whether spontaneous or medically terminated pregnancy′s. [22],[23],[24],[25],[26],27 We report 27.7% positivity in our study. It is this group that forms a high risk population and requires screening to avoid post abortal complications like PID, ectopic pregnancy and secondary infertility. Yashodhara[22] reports a very high incidence of 38.5% in her study, which was based on detection of IgM and IgG antibodies. Women experiencing recurrent spontaneous abortions have high titres of anti chlamydial IgG but negative endocervical cultures for C. trachomatis.[26] EIA technique for detection of Chlamydia antigen provides another alternative to culture. The reported sensitivity and specificity of these tests for genital infections (as compared to culture) have been 60-80% and 97-99% respectively in high risk populations. EIA offers the potential advantage over direct fluorescence assay (DFA) of objectivity and ease of mechanisation. It also allows batch processing, which is more conclusive in large scale screening. The best EIAs seem to have sensitivity similar to that of DFA in expert hands. However, non-culture tests are subject to false positive results. They should therefore be used with caution in low prevalence settings. Consequently, the interpretation of a positive test result must be handled with care and verification may be desirable. Verification of a positive test can be by either culture or a non culture test that identifies a different Chlamydia antigen, or nucleic acid sequencing or a blocking antibody or, a competitive probe. Cell culture technique for isolation of C. trachomatis are available mostly in large medical centers. The disadvantage of this being, limited availability, low and variable level of sensitivity (60-80%), its requirement for vigorous transport conditions and its high cost and technically demanding nature. Assays using nucleic acid probes like ligase chain reaction (LCR) and polymerase chain reaction (PCR) are also being used, which provides approximately equal results to the best of EIAs in terms of sensitivity and specificity. These tests are now the most sensitive diagnostic methods available for detecting Chlamydia infection, being the first non culture assay actually to surpass culture in sensitivity. The ability of these tests to detect Chlamydial genes in urine with high degree of sensitivity and specificity allows their use with urine specimens rather than the conventional urethral and cervical swabs. The use of urine sample is particularly appealing for Public-Health Chlamydia Screening Programmes. However, these tests require trained manpower, expensive equipment and perfect infrastructure; they are expensive to be used for screening purposes in developing countries like ours. In conclusion, the present study gives us an insight into the overwhelming problem of C. trachomatis infection. It is required that all the high risk pregnant women (previous history of abortions) are screened by this simple and reliable antigen detection test using ELISA technique and the positive result be verified by antibody blocking assay. The two methods in conjunction give results comparable to other methods used for diagnosis. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06029t1.jpg] [mb06029t2.jpg] [mb06029f2.jpg] [mb06029f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}