 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
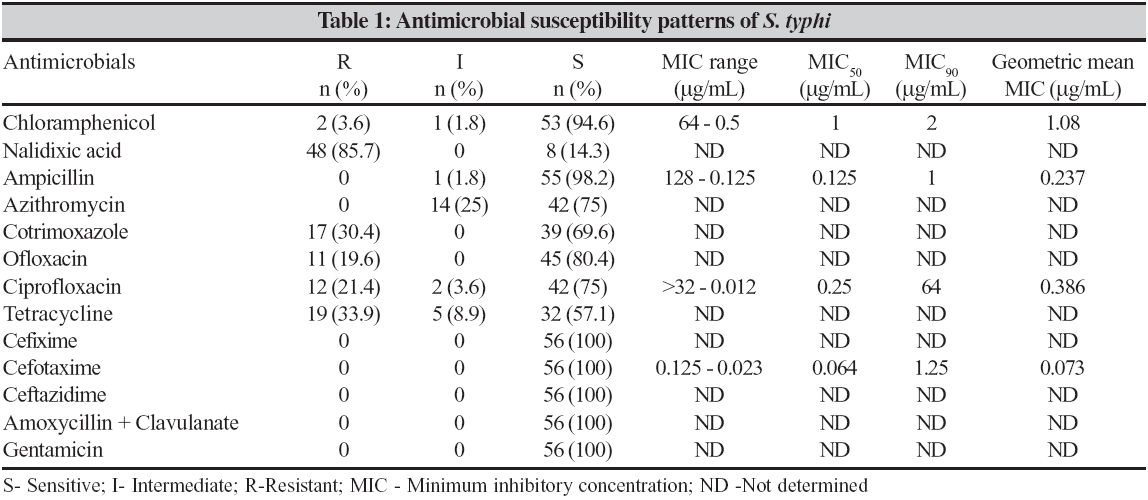
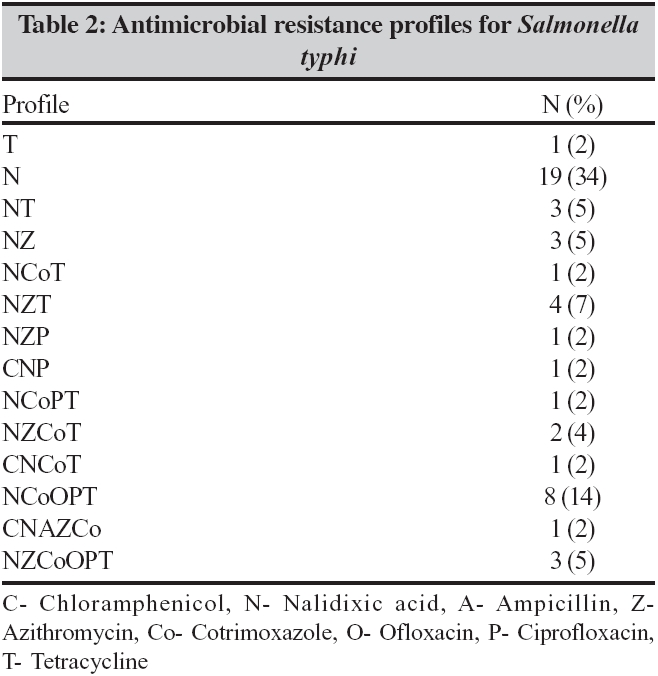
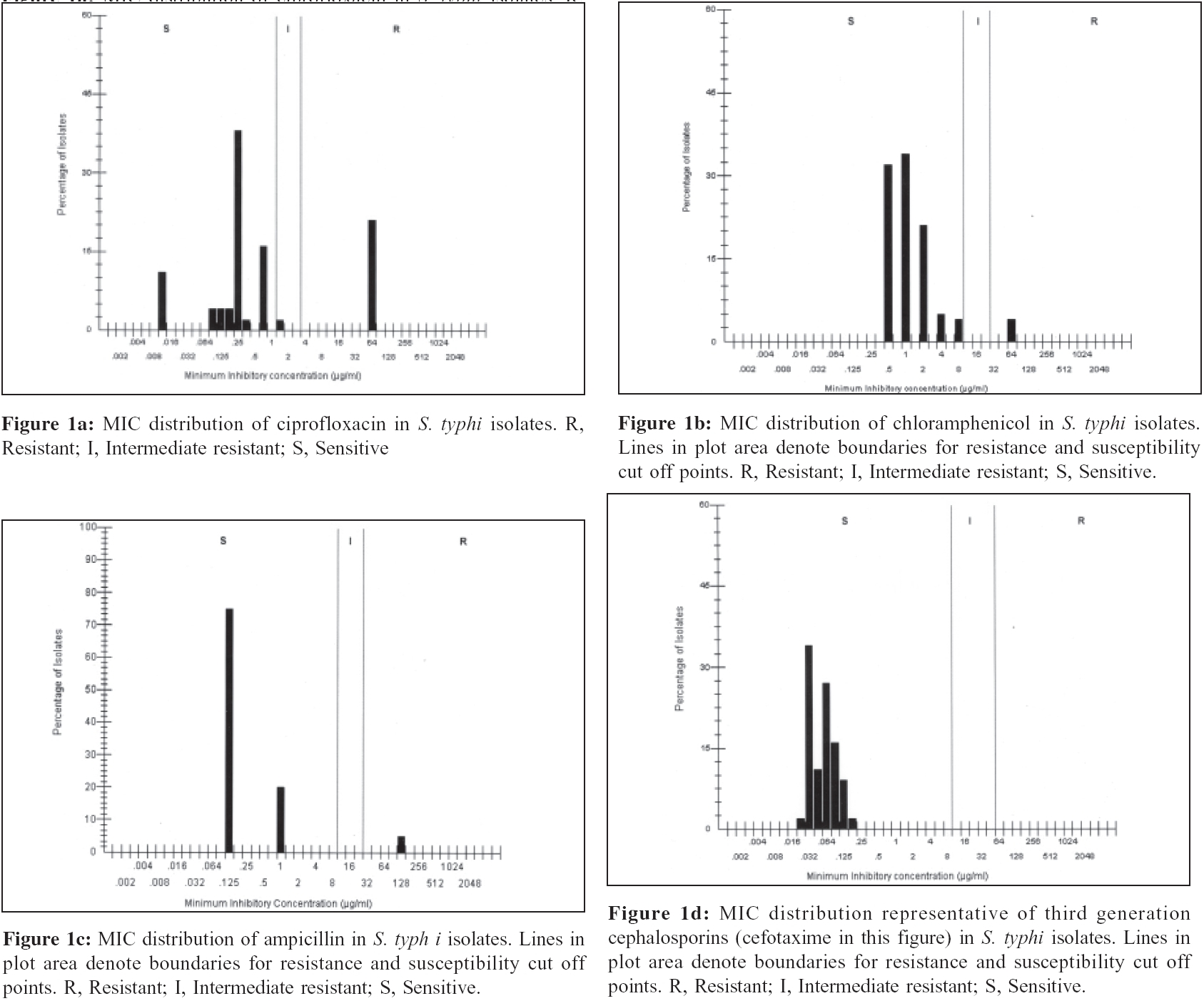
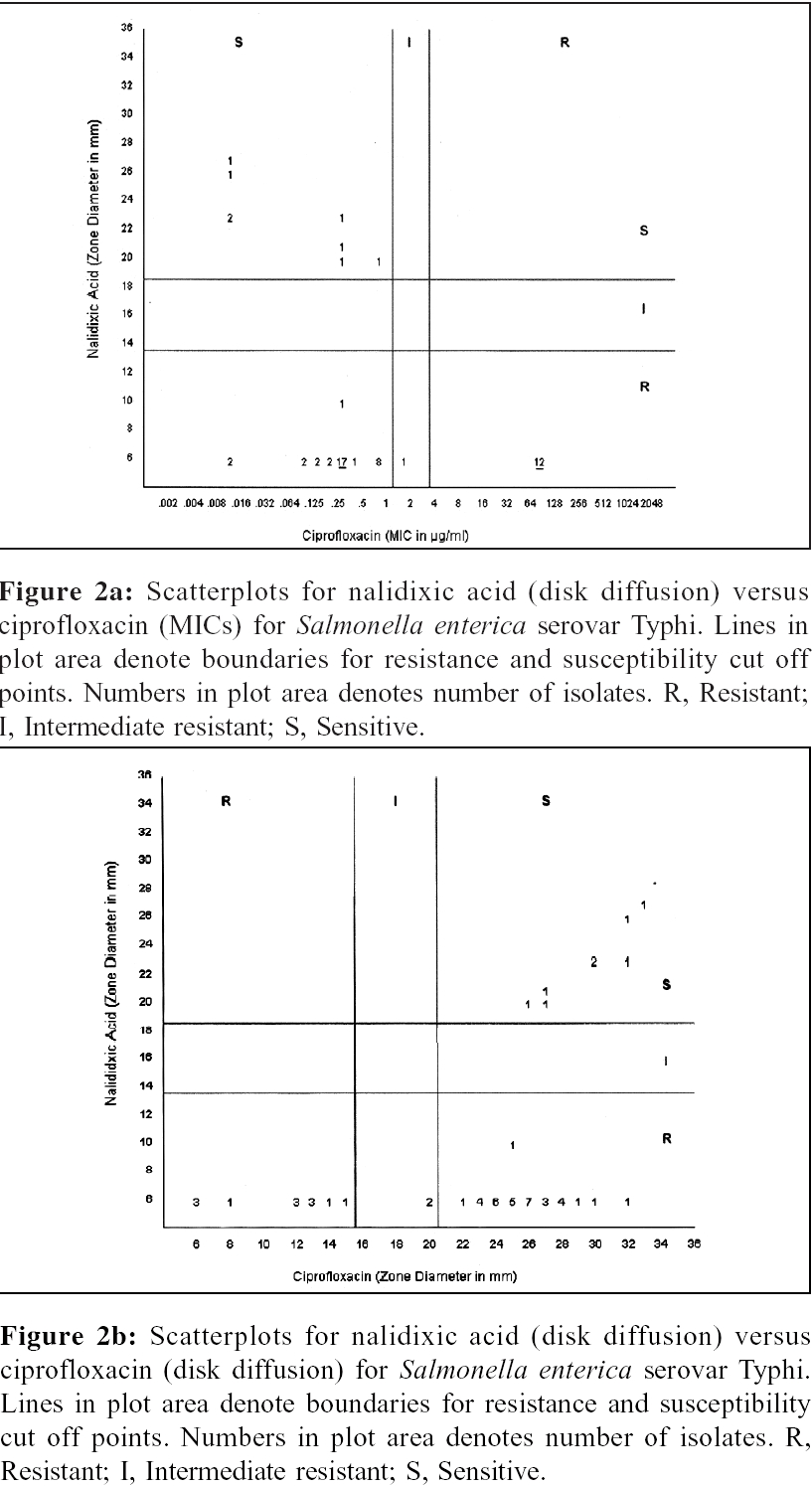
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 101-106 Original Article Treatment of enteric fever in children on the basis of current trends of antimicrobial susceptibility of Salmonella enterica serovar typhi and paratyphi A *Manchanda V, Bhalla P, Sethi M, Sharma VK Department of Clinical Microbiology, Maulana Azad Medical College and Associated Chacha Nehru Children Hospital, Geeta Colony, New Delhi - 110 031 Code Number: mb06030 Abstract Purpose: Recent reports indicate decreased susceptibility of S. typhi to fluoroquinolones, especially ciprofloxacin. Chloramphenicol has been suggested as first line therapy of enteric fever in many studies. This is a prospective study that describes the trends of antimicrobial susceptibility of S. typhi and S. paratyphi A causing bacteraemia in children and reports therapeutic failure to ciprofloxacin and evaluates the possible use of chloramphenicol, ampicillin, ciprofloxacin and third generation cephalosporins as first line therapy in the treatment of enteric fever in children. Keywords: Enteric fever, Salmonella, chloramphenicol, fluoroquinolones Multidrug resistant (MDR) strains (resistant to chloramphenicol, ampicillin and cotrimoxazole) of Salmonella enterica serovar Typhi ( S. typhi ) are increasingly being reported from India and worldwide.[1],[2],[3],[4] Third-generation cephalosporins and fluoroquinolones have been found effective in treatment of these cases.[5],[6] However, isolates of S. typhi with reduced susceptibility to fluoroquinolones (as indicated in the laboratory by resistance to nalidixic acid) have now appeared in the Indian subcontinent and other regions.[7],[8],[9],[10],[11],[12] These nalidixic acid resistant but ciprofloxacin sensitive strains have increased minimum inhibitory concentrations (MICs) for ciprofloxacin, although they are still within the current NCCLS range for susceptibility (0.12-0.5 mg/ml).[13] Therapeutic failures to ciprofloxacin have been reported in these cases of typhoid fever.[13],[14],[15] Furthermore, an isolate of S. typhi from Bangladesh with high-level resistance to ceftriaxone has already been reported.[16] However, reemergence of chloramphenicol susceptible strains have also been reported during recent years.[17],[18] A prospective study was planned to study the extended patterns of antimicrobial susceptibilities of S. typhi and S. paratyphi A isolated from the blood cultures at our hospital. Additionally, clinical therapeutic responses were observed for few of these cases to ciprofloxacin, ampicillin and cefixime. Also, the possible use of chloramphenicol, ampicillin, ciprofloxacin and third generation cephalosporins as first line therapy in the treatment of enteric fever in children was evaluated. Materials and Methods The study was conducted at Chacha Nehru Superspeciality Children Hospital, Delhi from May 2004 to April 2005. Blood samples of 673 children with suspected enteric fever were subjected to blood culture. Salmonella enterica serovar Typhi was isolated in 56 cases (8.3%) and Salmonella enterica serovar Paratyphi A in five (0.7%) cases. Antimicrobial susceptibility patterns were determined using following commercial antimicrobial disks (HiMedia, India): chloramphenicol (30 μg), nalidixic acid (30 μg), ampicillin (10 μg), azithromycin (15 μg), cotrimoxazole (1.25/23.75 μg), ofloxacin (5 μg), ciprofloxacin (5 μg), tetracycline (30 μg), cefixime (5 μg), cefotaxime (30 μg), ceftazidime (30 μg) amoxycillin + clavulanic acid (20/10 μg) and gentamicin (10 μg). Antimicrobial susceptibility testing was performed in accordance with the National Committee for Clinical Laboratory Standards (NCCLS) methodology.[19] Minimum inhibitory concentrations (MICs) for ciprofloxacin and cefotaxime were determined using E - test (AB Biodisk, Solana, Sweden). Broth microdilution testing was performed to determine MICs for chloramphenicol and ampicillin in accordance with the National Committee for Clinical Laboratory Standards (NCCLS).[20] The reagent powders were dissolved in Mueller-Hinton broth and distributed to the wells of microdilution trays. Each tray was inoculated with 5×10 4 CFU per well to yield a final volume of 0.1 ml per well. Final dilutions ranged from 256 μg/mL - 0.25 mg/mL. The trays were incubated overnight at 35°C. Quality control was monitored by using Escherichia coli ATCC 25922. The recorded MIC of each antibiotic was the lowest concentration that completely inhibited visible growth of the test strain. The MIC at which 50% of the isolates tested were inhibited (MIC50) and MIC90 were calculated in accordance with the current NCCLS methodology and using WHONET software ver 5.1. Results All 56 isolates of S. typhi were found sensitive to amoxycillin + clavulanate combination, gentamicin, cefixime, cefotaxime and ceftazidime. Details of antimicrobial susceptibility patterns are shown in [Table - 1]. Seven S. typhi isolates were sensitive to all drugs tested. Two isolates showed resistance to chloramphenicol. Multi-drug resistance (MDR, resistant to ≥ 3 drugs) was observed in 22 cases (39%) and resistance to ≥ 5 drugs was seen in 12 cases (21%). All five S. paratyphi A isolates were sensitive to ampicillin and chloramphenicol and resistant to nalidixic acid. Fourteen different types of antimicrobial profiles were observed for S . typhi . Nineteen isolates were resistant only to nalidixic acid (N), three each were additionally resistant to azithromycin (NZ) and tetracycline (NT). Eight isolates were found resistant to nalidixic acid, cotrimoxazole (Co), ofloxacin (O), ciprofloxacin (P) and tetracycline (T) (NCoOPT). Detailed antimicrobial resistance profiles are summarized in [Table - 2]. Five S. paratyphi A isolates had three different resistance profiles. Three isolates were resistant to nalidixic acid and azithromycin (NZ) and one isolate each was resistant to nalidixic acid alone (N) and to nalidixic acid and tetracycline (NT). Seven (13%) strains were sensitive to all drugs. Minimum inhibitory concentrations (MICs) range and their distribution among the isolates are shown in [Table - 2] and [Figure - 1]a-d. Nalidixic acid resistant S. typhi (NARST) isolates were obtained in 48 cases and nalidixic acid sensitive isolates were found among eight cases of suspected typhoid fever. Among NARST, only 12 isolates met the criteria of current NCCLS break points for ciprofloxacin resistance and only two isolates had MIC < 0.12 μg/mL. The remaining 42 isolates had increased MICs between ≥ 0.12 - < 1 μg/mL [Figure - 2]a and b. Scatter plot [Figure - 2]a compares nalidixic acid zone diameters and ciprofloxacin MICs. Large numbers of isolates were found in the area of nalidixic acid resistance with slightly increased MICs for ciprofloxacin (0.12 -1 μg/mL), but still below the current break point (< 1 μg/mL). Another scatter plot [Figure - 2]b compares nalidixic acid zone diameters with that of ciprofloxacin zone diameters. In this figure, majority of the isolates fall in nalidixic acid resistant but ciprofloxacin sensitive area. Among S. paratyphi A isolates, MIC for ciprofloxacin ranged between 0.125-0.75 μg/mL and for chloramphenicol ranged between 0.5-8 μg/mL. MIC distribution for cefotaxime was between 0.064-0.094 μg/mL. All five isolates had MIC of 1.0 μg/ml for ampicillin. Oral ciprofloxacin (10 mg/kg/day) was prescribed to the first five patients infected with nalidixic acid resistant but ciprofloxacin sensitive S. typhi (MIC > 0.64 μg/mL but < 1 μg/mL) and were reviewed after five days. Of these five patients, only one responded to the therapy. In the remaining four patients, higher doses of ciprofloxacin (20 mg/kg/day) were advised and they were reviewed after another three days. Only two of them responded by this time. Oral cefixime (16 mg/kg/day) was advised in the other two and an excellent response was observed. During the rest of the study none of the culture positive patients of typhoid fever were advised ciprofloxacin. They were advised either oral amoxycillin (100 mg/kg/day) or cefixime (20 mg/kg/day) to which, they responded well. The follow up was uneventful. Discussion In the preantibiotic era, typhoid fever case fatality rates approached 20%. Treatment with effective antimicrobial agents - ampicillin, chloramphenicol, cotrimoxazole and later ciprofloxacin - has reduced the case fatality rate to less than 1%.[21] The resistance pattern for S. typhi varies with geographical locations. Many studies have suggested that patients in Indian subcontinent or with the history of travel to the Indian subcontinent should receive ciprofloxacin as first line therapy.[8],[22] However, S. typhi isolates resistant to ciprofloxacin and ceftriaxone (MIC, 64 mg/L) have been reported.[13],[16],[23],[24],[25],[26],[27] S. typhi strains with reduced susceptibility to fluoroquinolones have become a major problem in Asia and other parts of the world.[12] Although they were reported to be susceptible to fluoroquinolones, by disk testing with the use of recommended break points, these organisms were resistant to nalidixic acid and the MIC of fluoroquinolones for these strains was 10 times higher than that for fully susceptible strains. This reduction in susceptibility results in a poor clinical response to treatment. There is unpredictable response to treatment with ciprofloxacin in patients infected with these kinds of S. typhi strains. Selective pressure on the bacterial population by uncontrolled use of quinolones has likely led to emergence of resistance to this group of antimicrobials. This has been attributed to point mutation in quinolone resistance determining region (QRDR) of the topoisomerase gene gyr A, characteristically occurring at position 83 of the DNA gyrase enzyme (changing serine to phenylalanine) and position 87 (changing aspartate to tyrosine or glycine).[9] However, other mechanisms of resistance such as decreased permeability and active efflux of the antimicrobial agent may be involved. In other Enterobacteriaceae , higher levels of quinolone resistance have been associated with additional mutations in the gyr A gene, mutations in other topoisomerase genes, or alterations in fluoroquinolone uptake.[13] No such mutations have been reported yet in S. typhi , although there are sporadic reports of completely fluoroquinolone resistant isolates. Because clinical response to fluoroquinolones in patients infected with nalidixic acid resistant strains is greatly inferior to the response in those infected with nalidixic acid-susceptible strains, the break points for the classification of S.typhi strains according to their susceptibility to fluoroquinolones should be reviewed. A practical approach would be to classify strains that are resistant to nalidixic acid but susceptible to fluoroquinolones according to current disk testing criteria as resistant to quinolones or non susceptible to fluoroquinolones as suggested by other authors as well.[12] All strains that have intermediate susceptibility or resistance to fluoroquinolones on disk testing (as defined by NCCLS guidelines) should be considered fluoroquinolone resistant. There are reports that show that treatment of patients infected with similar isolates is at potential risk of therapeutic failure.[13] This study showed that resistance to nalidixic acid is generally associated with increased MICs of ciprofloxacin. Hence, nalidixic acid susceptibility testing must be included with ciprofloxacin susceptibility testing in routine microbiological laboratory. Treatment with ciprofloxacin must be avoided in nalidixic acid resistant isolates of S. typhi although higher doses may be helpful in a few cases. Most of the isolates in this study were found susceptible to chloramphenicol and ampicillin. Percentage resistance, intermediate resistance and sensitive (%RIS) data in [Table - 1] show that ampicillin and chloramphenicol should be considered for the treatment of typhoid fever in children in Delhi, however, MIC distribution data projects different scenario. As discussed above, infection with isolates with raised MICs but still in susceptible range for ciprofloxacin [Figure - 1]a has a potential risk of therapeutic failure. MIC distribution of chloramphenicol closely resembles that of ciprofloxacin in raised MICs but still in susceptible range [Figure - 1]b. Hence, theoretically, treatment with chloramphenicol also has a potential risk of therapeutic failure. More studies are needed to evaluate reuse of chloramphenicol as the first choice for treatment of typhoid fever. Minimum inhibitory concentrations of ampicillin and cefixime on the other hand were well below the susceptible limits and hence may be used safely in the treatment of typhoid fever. To conclude, MIC distribution for ciprofloxacin and chloramphenicol had striking similarity, i.e, raised MICs but still in susceptible range. However, MICs distribution of ampicillin and cefotaxime was well below the susceptible limits. Therapeutic failures for ciprofloxacin have been observed. Similar responses may be observed for chloramphenicol. Therapeutic choice for typhoid fever should be carefully selected. Ampicillin and probably not chloramphenicol may be reconsidered as first line of therapy in uncomplicated cases of typhoid fever in children. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06030f2.jpg] [mb06030t1.jpg] [mb06030f1.jpg] [mb06030t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}