 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
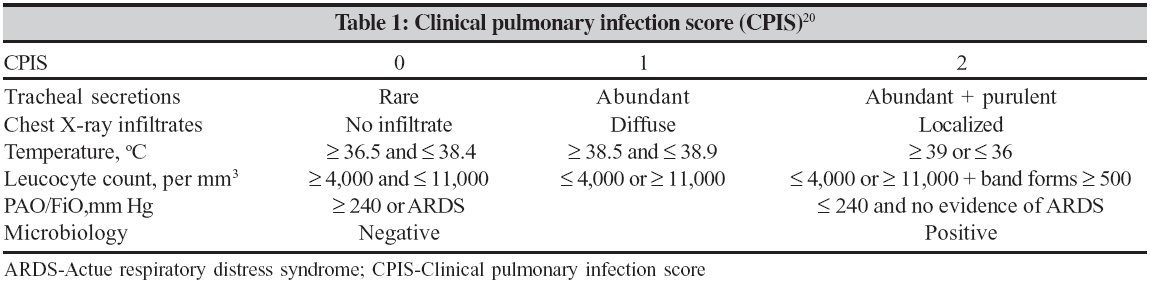
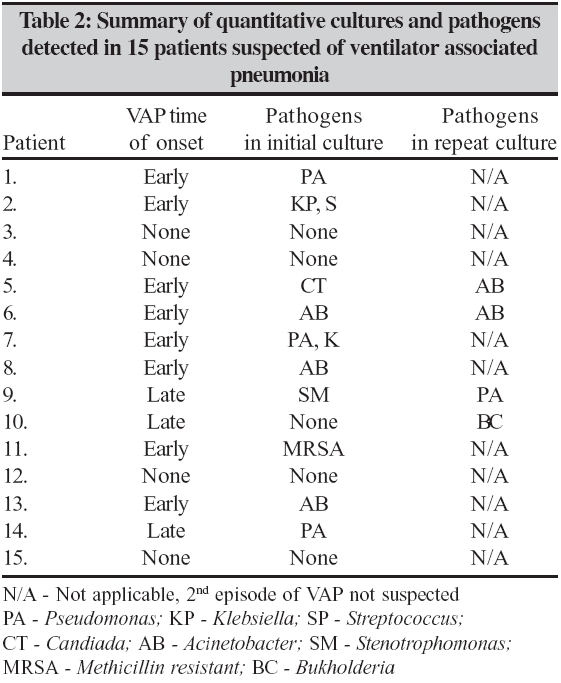
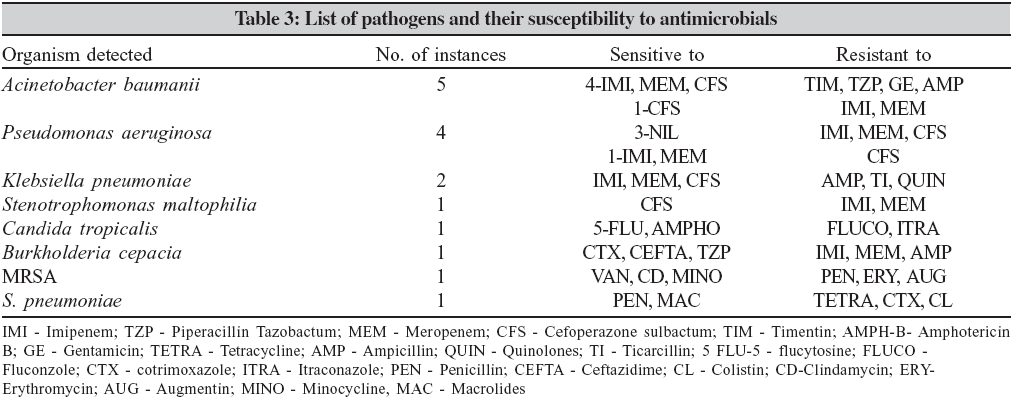
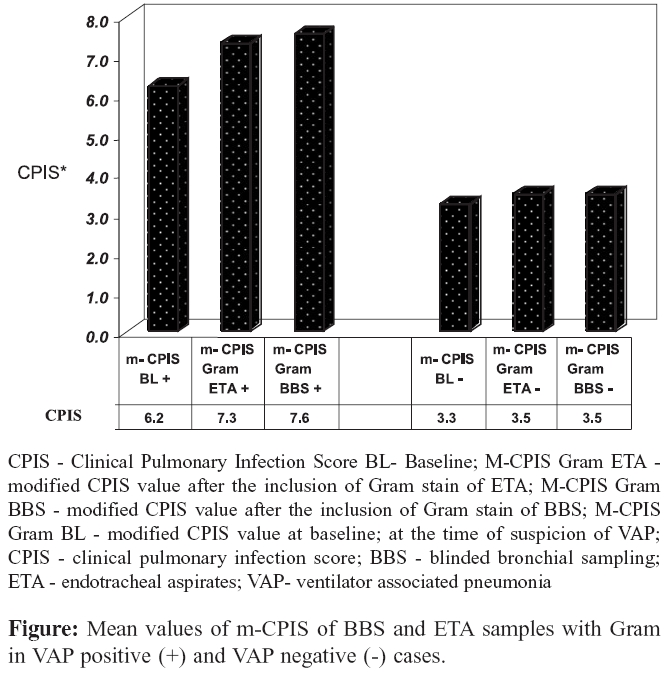
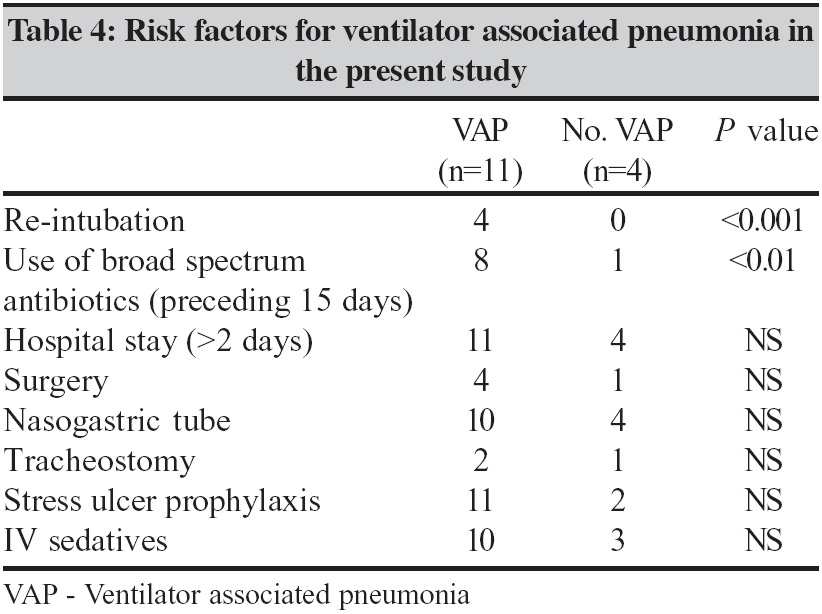
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 107-113 Original Article The role of quantitative cultures of non-bronchoscopic samples in ventilator associated pneumonia Rajasekhar T, Anuradha K, Suhasini T, *Lakshmi V Department of Microbiology, Nizam's Institute of Medical Sciences, Punjagutta, Hydearabad - 500 062, AP Code Number: mb06031 Abstract Purpose: The objective of this study is to determine the role of quantitative cultures of non-bronchoscopic samples such as blinded bronchial sampling (BBS) and endotracheal aspirates (ETA) in the management of ventilator associated pneumonia (VAP). The study also evaluates the clinical diagnosis of VAP based on the inclusion of Gram stain results of BBS/ETA samples into modified clinical pulmonary infection score (CPIS).Methods: Fifteen out of the 120 patients admitted to respiratory intensive care unit under mechanical ventilation for more than 48 hours with a clinical suspicion of VAP, were included in this study. Quantitative cultures of BBS and ETA were performed from all the 15 patients. Results: VAP was confirmed in 11 out of 15 cases by quantitative cultures of either the BBS or ETA samples. The condition of 8/11 VAP confirmed patients improved significantly with the change in antibiotic therapy. The overall mortality rate was found to be 18%. The agreement between BBS and ETA results was found to be 83.3%. Modified-clinical pulmonary infection score (CPIS) increased significantly when Gram stain results of BBS/ETA samples were included, thereby strengthening the clinical diagnosis of VAP. Conclusions: Quantitative culture of lower respiratory tract samples obtained by non-bronchoscopic methods may be a useful alternative to bronchoscopy, in the diagnosis of VAP. Inclusion of Gram stain results of BBS/ETA into modified-CPIS may augment the diagnostic evaluation of VAP. Keywords: Quantitative cultures, blinded bronchial sampling, clinical pulmonary Infection score, ventilator associated pneumonia Ventilator-associated pneumsonia (VAP), an important form of hospital acquired pneumonia (HAP), specifically refers to pneumonia developing in a mechanically ventilated patient more than 48 hours after tracheal intubation or tracheostomy. VAP continues to complicate the course of patients receiving mechanical ventilation in spite of major advances in techniques for its diagnosis and treatment. VAP requires a rapid diagnosis and initiation of the appropriate antibiotic treatment since many studies have shown the adverse effect of inadequate antibiotic treatment on the patients′ prognosis.[1] Detection of the causative organism is crucial for the diagnosis of VAP. This is done by microbiological investigation wherein samples (bronchoscopic/non-bronchoscopic) obtained from the lower respiratory tract are cultured quantitatively or semi quantitatively. The major difficulty of this approach is in obtaining samples from the lower respiratory tract mainly because of its probable contamination with the upper airway flora, which may result in misinterpretation of cultures. The American thoracic society (ATS) guidelines recommend that quantitative cultures can be performed on endotracheal aspirates or samples collected either bronchoscopically or non-bronchoscopically.[2] At the present time, bronchoscopic sampling of the lower airways, using either a protected specimen brush (PSB) or bronchoalveolar lavage (BAL) is accepted as the most accurate method of diagnosing VAP, short of direct tissue examination. However, bronschoscopy is not readily available in many settings and there is a growing need to evaluate other sampling techniques for collecting respiratory secretions. The collection of blind, non-bronchoscopic samples is an appealing alternative. Blind sampling can be done by BAL, PSB, or a blind bronchial suction sample (BBS) can be taken.[3] In addition, they require less expertise and may thus be more readily available. There are many studies, which compared the diagnostic value of quantitative cultures of bronchoscopic and non-bronchoscopic samples in VAP whereas little data is available from Indian population.[4] Therefore, this study was aimed at evaluation of the usefulness of quantitative cultures of non-bronchoscopic samples in the management of VAP in the respiratory intensive care unit (RICU) of a tertiary care hospital. In most hospitals in India, qualitative or semi-quantitative cultures of endotracheal aspirates are routinely performed for the management of VAP. Reliance on semiquantitative cultures, which may not reliably separate true pathogens from colonizers, can lead to either more or broader spectrum antibiotic therapy than with a quantitative approach.[2] Hence, quantitative cultures are preferred to semiquantitative cultures for the diagnosis of VAP. VAP may also be managed by the clinical approach, which underlines prompt empiric antibiotic therapy for all patients suspected of having VAP. The presence of pneumonia is defined by new or progressive radiographic infiltrate plus atleast 2 of 3 clinical features (temp> 38°C / < 35°C, leucocytosis / leucopenia and purulent tracheal secretions).[5] This approach avoids the problem of not treating some infected individuals. However, the major drawback is that it is overly sensitive and leads to more antibiotic therapy as compared to therapy decisions based on the microbiological findings.[6] Clinical pulmonary infection score (CPIS) was introduced by Pugin et al[7] as a diagnostic tool for VAP, which includes microbiological data into the clinical criteria for diagnosis. This cannot be used for screening VAP as culture results are not immediately available. Singh et al[8] modified the CPIS by excluding microbiological data from the scoring (hereafter referred to as modified-CPIS or m-CPIS in this article). They observed that the empiric antibiotic treatment could be stopped on day 3 if the scoring on m-CPIS is < 6 and can be continued for the entire course if m-CPIS is > 6. This current study was also aimed at evaluation of m-CPIS as a diagnostic tool for VAP after incorporating Gram stain results of ETA and BBS samples from patients suspected of having VAP. Materials and Methods Patients All patients suspected of having VAP were observed daily and data were compiled that included age, gender, date of admission in RICU, underlying disease, date of intubation/tracheostomy, duration of mechanical ventilation before inclusion in the study, date of inclusion in the study and modified CPIS. Days of antibiotic therapy and a short description of radiological findings were recorded. Patients were monitored from the time of inclusion in the study to the date of discharge from RICU. The patients were divided into two groups, ′early-onset VAP′ and ′late-onset VAP′. The classification was done based on the duration of mechanical ventilation until the day of clinical suspicion of VAP. Patients on mechanical ventilation for less than 5 days were included in the early-onset group and the rest were included in the late onset group. Resolution of the disease in the patients was defined as clinical improvement accompanied by normal temperature, decreased volume and transparency of tracheobronchial secretion and radiologically confirmed elimination of the infiltrate. Once clinical suspicion was established, empiric antibiotic therapy was initiated based on the guidelines prescribed by American Thoracic Society (ATS). After the quantitative culture results of BBS and ETA were obtained, the antibiotics were changed accordingly. Specimen collection Processing Calculation of m- CPIS and m- CPIS gram Interpretation of quantitative culture results Patient follow-up Results Results of the quantitative cultures The analysis and outcome of the quantitative culture for the 11 patients tested positive for ETA/BBS is summarized in [Table - 2] . Nine patients had infection with only one type of microorganism. Four out of nine patients were suspected to have a second episode of VAP and a repeat culture was performed. One of these four patients had tested negative for VAP initially with the first culture. In the other three patients with a repeat episode of VAP, a single organism was found in the repeat culture. A total of 16 organisms were isolated above the diagnostic thresholds by either of the two sampling techniques from the 11 culture positive cases. As seen in [Table - 2], the most frequently isolated organisms were Acinetobacter baumanii and Pseudomonas aeruginosa. The predominant organisms in the early-onset VAP group were Acinetobacter baumanii and Klebsiella spp. In the late onset group Pseudomonas aeruginosa was the most predominant. The spectrum of pathogens isolated in the current study can be seen in [Table - 3] and their susceptibility patterns. Agreement between ETA and BBS cultures M-CPIS analysis Similarly, the mean m-CPIS Gram of the ETA sample increased in VAP positive and negative cases. As seen in the [Figure - 1] the difference between m-CPIS Gram of ETA sample (7.33±1.73) and m-CPIS baseline (6.22±1.39) was significant in VAP positive cases ( P < 0.05) where as the difference in VAP negative cases was not significant. On comparison of m-CPIS Gram BBS with m-CPIS Gram ETA, no significant difference was observed in both VAP positive and negative cases. As compared with the m-CPIS baseline, the accuracy of the m-CPIS Gram of both BBS and ETA samples in distinguishing between VAP positive and negative cases thus increased after the inclusion of Gram stain into the score. Risk factor analysis Clinical outcomes of the patients Discussion VAP is one of the major complications in the ICU patients, the mortality rates from which can range from 25 to 50%.[4] The risk of VAP is highest early in the course of hospital stay and is estimated to be approximately 3% per day during the first five days of ventilation, approximately 2% per day during days 5 to 10 of ventilation and approximately 1% per day thereafter.[10] It is therefore essential to have a high degree of suspicion of VAP in the first week after intubation. The pathogenesis for VAP is related to host and treatment related colonization factors. Aspiration of oropharyngeal pathogens and the leakage of secretions containing bacteria around the endotracheal tube are principal factors for the development of VAP.[11] The progression from colonization to tracheobronchitis to VAP is a dynamic equilibrium. Diagnostic testing in VAP is necessary as it allows one to define whether a patient has pneumonia as the reason for a set of signs and symptoms and to find out the etiologic pattern when pneumonia is present. The bacteriological approach for the management of VAP avoids the problem of over treatment by separating colonizers from infecting pathogens. Several methods to avoid contamination have been proposed like the use of invasive bronchoscopic methods and bronchial biopsy for sampling from the site of infection and a protected specimen brush. These methods have been shown to be highly specific in diagnosing VAP.[12] However, bronchoscopy is not accessible in many settings and because of the invasive nature and cost of the bronchoscopy, investigators have evaluated other techniques for collecting lower respiratory tract secretions. Several methods to obtain good respiratory samples have been extensively investigated; each technique having its own diagnostic threshold and methodological limitations. The choice of method depends on expertise, experience, availability and cost. Ruiz et al[13] showed that patient outcomes were similar irrespective of the method used for diagnosis (bronchoscopic or endotracheal aspiration). Some studies[14] also showed that the results of quantitative cultures of endotracheal aspirates were comparable to those using invasive bronchoscopic methods. Blinded bronchial sampling or blind bronchial suction (BBS) is a nonbronchoscopic technique where the sample is taken directly from the bronchial region by blindly passing the catheter through the endotracheal tube and wedging into a bronchus. Papazian et al[15] showed that the sensitivity of BBS was significantly higher than that of PSB and it is a simple, repeatable and risk free procedure for obtaining culture specimens from mechanically ventilated patients. There are very few studies on the evaluation of utility of BBS in VAP. In our current investigation, we evaluated the efficacy of blinded bronchial sampling in the management of VAP. One of the most important findings of this study is that the quantitative culture of lower respiratory tract samples obtained by the non-bronchoscopic techniques is highly useful in early diagnosis and appropriate treatment of VAP. We tested two types of non-bronchoscopic sampling techniques, BBS and ETA in a group of 15 patients with clinical suspicion of VAP. We could detect VAP in 11 patients in whom the quantitative cultures of either BBS/ETA or both showed pathogens most commonly responsible for VAP. A. baumanii and Pseudomonas aeruginosa were the most commonly isolated organisms both of which are potentially drug resistant. Our current study showed that A . baumanii was isolated in all instances from the samples of the early-onset VAP group of patients. In contrast, Trouillet et al[16] found that VAP due to potentially drug resistant organisms was more common in the late-onset group of patients who received prior antibiotic therapy. The emergence of these potentially drug resistant organisms in the early-onset group in our study may be attributed to the prior use of broad-spectrum antibiotics ( P < 0.01), which was one of the significant risk factors associated with the development of VAP [Table - 4]. The other potentially drug resistant organisms isolated were Stenotrophomonas maltophilia and methicillin resistant S taphylococcus aureus (MRSA), both of which were also found in the early-onset group. Eight of these patients showed significant clinical improvement with the modified antibiotic therapy, which confirms their recovery from VAP. Two patients died during the course of the treatment and both these patients belonged to the late-onset VAP group in whom multi drug resistant P. aeruginosa was isolated. We also observed that the death rate associated with Pseudomonas VAP was 50%. Death rates associated with Pseudomonas VAP have been observed to be 70-80% in some studies.[17] Both the non-bronchoscopic techniques, BBS and ETA were found to be safe and useful. Together, the samples helped in detecting pathogens responsible for causing VAP in 11 out of the 15 patients suspected of VAP. VAP was confirmed by a correlation between positive quantitative culture results and the clinical outcome of patients. The application of quantitative thresholds to cultures obtained from non-bronchoscopic samples is necessary to improve their overall diagnostic specificity, due to the presence of tracheobronchial colonization. The quantitative cultures were considered positive for a diagnostic threshold of 10 5 cfu/mL for ETA samples and 10 4 cfu/mL for BBS samples. All patients with clinical suspicion of VAP were given empiric antibiotic therapy before the culture results were obtained. Therefore the diagnostic thresholds for ETA and BBS cultures were adjusted to colony counts of 10 5 cfu/mL and 10 4 cfu/mL respectively. Jourdain et al[18] have attempted to establish a cut off for assigning significance to colony counts in endotracheal aspirates by examining sensitivity, specificity and overall accuracy. They concluded that a level of 10 5 to 10 6 cfu/mL of the exudate was optimal for diagnostic purposes. With counts higher than this there was a significant decrease in sensitivity although the specificity remained high. In this study, since all the patients received antibiotics prior to the investigation, a colony count of 10 5 cfu/mL was considered the diagnostic threshold for the ETA samples. For BBS samples there are no standardized diagnostic thresholds and hence we considered a colony count of 10 4 cfu/mL as the diagnostic threshold as done by other investigators.[15],[19] The culture results of BBS were found to be more sensitive than those of bronchoscopic techniques such as PSB and BAL in diagnosing VAP. But, there is also a need to study the impact of quantitative cultures of BBS on the clinical outcomes of the patients. Based on clinical outcome of patients, few studies have evaluated the utility of BBS in VAP. Papazian et al owed that results of semi quantitative cultures of BBS samples were comparable to those of PSB and BAL.[15] In another study Papazian et al compared the results of BBS, mini-BAL, BAL and PSB with histology and culture of lung tissue specimens and found that the sensitivity of BBS was significantly higher than that of PSB.[19] This study is similar to the one undertaken by Fartoukh et al who showed that adding Gram stain results of lower respiratory samples to the m-CPIS increased its specificity and sensitivity in diagnosing VAP.[20] They used bronchoscopy for sampling of the airways. We used the non-bronchoscopic techniques, BBS and ETA for sampling of the lower airways, The advantages of using lower airway samples obtained by non-bronchoscopic techniques for m-CPIS Gram are that these techniques are readily available, safe and easy to execute and comparatively cost effective. Papazian et al found that at a threshold of six, the sensitivity and specificity of CPIS was found to be 72% and 85% when compared with histology and lung tissue specimens as reference standard, but at a threshold of 10, when CPIS was combined with the logarithmic concentration of the predominant microorganism obtained from the BBS sample the specificity increased to 95%.[19] In our study the mean m-CPIS Gram of BBS sample value of 7.55 was significantly higher than the mean m-CPIS baseline value of 6.22 in the patients who were VAP positive ( P < 0.01). Likewise, the mean m-CPIS Gram of ETA was 7.33 and significantly higher than mean m-CPIS baseline value of 6.22 in the VAP positive patients ( P < 0.05). While they used bronchoscopy as the reference standard for testing the accuracy of m-CPIS Gram for diagnosing VAP, we considered the clinical outcome of the patients as the reference standard. During the course of our study we evaluated the important risk factors associated with the development of VAP in all patients suspected of VAP. Independent risk factors for VAP that were identified by multivariate analysis were considered.[4] In our setting we could identify two significant risk factors associated with the development of VAP i.e, re-intubation with a P < 0.001 and prior use of broad spectrum antibiotics with a P < 0.01 [Table - 4]. The identification of these modifiable risk factors is necessary in estimating the probability of lung infection in the intensive care patients so that effective preventive measures can be taken to decrease the likelihood of occurrence of VAP in this group of patients. These two risk factors were also found to be significant in a study done by Pawar et al in a cardiac surgical ICU.[21] They identified re intubation and prior use of antibiotics as two of the many significant risk factors with univariate analysis. This affirms that preventive measures should be taken to reduce the chances of reintubation whenever possible. It is well known now that prior use of broad spectrum antibiotics not only is responsible for VAP but also for the emergence of drug resistance. On comparison of the results of quantitative cultures of BBS and ETA, the agreement between the results of BBS and ETA was 83.3%. It is well known that BBS may be a better sample than ETA as the chances of contamination with the upper airway flora are less with BBS. Because of the small sample size, we could not find a significant difference between the results of BBS and ETA. Currently the data on BBS is scanty, so there is a need to study the utility of BBS in a larger population to gather more data on the usefulness of BBS and its impact on the clinical outcome of the patients. We did not test the sensitivity and specificity of BBS/ETA results, as it was not feasible to perform lung biopsy or autopsy, which is considered as the most acceptable reference standard. Bronchoscopy was not available and we used the clinical outcome of the patients as the reference standard by performing long-term follow up of the patients to exclude any other diagnosis. This study showed that quantitative cultures of lower respiratory tract samples obtained by non-bronchoscopic methods may be a useful alternative to bronchoscopy in the diagnosis of VAP. However, results from this study need to be validated by comparison to gold standards such as histology of lung tissue. This study also helped to identify the organisms most commonly responsible for VAP and the appropriate antibiotic therapy. BBS is a safe, easy and useful technique for routine microbial investigation of VAP when bronchoscopy is not available. Inclusion of Gram stain results of ETA/BBS into modified-CPIS may augment the diagnostic evaluation of VAP. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06031t4.jpg] [mb06031f1.jpg] [mb06031t3.jpg] [mb06031t2.jpg] [mb06031t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}