
|
Indian Journal of Medical Microbiology
Medknow Publications on behalf of Indian Association of Medical Microbiology
ISSN: 0255-0857 EISSN: 1998-3646
Vol. 24, Num. 2, 2006, pp. 117-120
|
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 117-120
Brief Communications
Comparison of double disc and three dimensional methods to screen for ESBL producers in a tertiary care hospital
*Menon T, Bindu D, Kumar CPG, Nalini S, Thirunarayan MA
Department of Microbiology, Dr. AL Mudaliar Post Graduate Institute of Basic Medical Sciences, University of Madras, Taramani, Chennai - 600 113
*Correspondence Address:Department of Microbiology, Dr. AL Mudaliar
Post Graduate Institute of Basic Medical Sciences, University of Madras,
Taramani, Chennai - 600 113, thangam16@rediffmail.com
Code Number: mb06033
Abstract
Extended spectrum β lactamases (ESBLs) continue to be a major problem in clinical setups world over, conferring resistance to the expanded spectrum cephalosporins. An attempt was made to study ESBL production among Enterobacteriaceae members from a tertiary care center in Chennai. A total of seventy randomly collected isolates of the family Enterobacteriaceae from a tertiary care center was studied for their susceptibility patterns to various antibiotics and detection of ESBL producers by double disc synergy (DDS) test and three dimensional test (TDT). Eighty percent of the isolates were multidrug resistant (MDR) and 20% were ESBL producers. TDT detected 85.7% whereas only 14.2% were detected by DDS. In the present study, a large number of isolates were found to be MDR and ESBL producers. TDTs were found to be better than DDS in the detection of ESBLs. Continued monitoring of drug resistance is necessary in clinical settings for proper disease management.
Keywords: Extended spectrum β lactamases, multidrug resistance, enterobacteriaceae
Extended (or expanded) spectrum β lactam antibiotics such as third generation cephalosporins (3GC) form the major component of the empiric antibacterial armamentarium in most clinical setups and especially in tertiary care centers.[1] Extensive use of 3GC has contributed to the evolution of ESBL (Extended spectrum β lactamases). These plasmid mediated groups of enzymes are the products of point mutations at the active site of TEM, SHV and OXA enzymes. The ESBL hydrolyze penicillins, extended spectrum cephalosporins with an oxyimino side chain including ceftazidime, ceftriaxone and cefotaxime and oxyimino-monobactam antibiotics such as aztreonam.[2] ESBL occur predominantly in Klebsiella spp. and Escherichia coli but have also been increasingly reported in other genera of the family Enterobacteriaceae .[3],[4] A plethora of ESBL has been identified accounting for resistance to oximino-cephalosporins. Till date, over 150 different ESBLs have been described.
The present study aimed at analyzing the susceptibility pattern of major Enterobacteriaceae members
namely Klebsiella spp, E. coli , Citrobacter spp.
and Enterobacter spp. from cancer patients attending a tertiary
care center in Chennai, South India and detect presence of ESBLs.
Materials and Methods
Setting and samples
Seventy clinical isolates of Enterobacteriaceae from cancer patients admitted in Apollo Speciality Hospital, a tertiary care center in Chennai, South India from March 2002 to December 2003 were studied. Thirty three isolates were Klebsiella spp, 26 E. coli , seven Enterobacter spp. and four Citrobacter spp. Twenty nine isolates were from urine, 13 from endotracheal aspirates, 12 from pus, six from sputa, four from blood, three from bronchial wash, two from aspiration fluid and one from vaginal swab. Identification of isolates was done based on cultural characteristics and reactions in standard biochemical tests.
Antibiotic susceptibility testing
The susceptibility of the isolates
was determined against 21 antibacterial agents by disc diffusion method.
They included cefazolin (Cz-30 µg), cefuroxime (Cu-30 µg), ceftriaxone (Ci-30 µg), cefotaxime (Ce-30 µg), ceftazidime (Ca-30 µg), ceftizoxime (Ck-30 µg), cefpirome (Cpo-30 µg), gentamicin (G-10 µg), tobramycin (Tb-10 µg), isepamicin (Ise-30 µg), amikacin (Ak-30 µg), netilmicin (Nt-30 µg), ofloxacin (Of- 5 µg), piperacillin (Pc-100 µg), imipenem (I-10 µg), aztreonam (Ao-30 µg), cefaperazone-sulbactum (Cs- 75/35 µg), cotrimoxazole (Co-25 µg), piperacillin-tazobactum (Pt-100 µg), tetracycline (T-30 µg) and chloramphenicol (C- 30 µg).
Susceptibility and resistance was determined based on the interpretative
criteria recommended by the National Committee for Clinical Laboratory
Standards (NCCLS).[5] E. coli ATCC
25922 was used as the quality control strain.
Tests for determination of ESBL activity
Double disk synergy method (DDS)
Test strains were preincubated in brain heart infusion broth (BHIB)
at 37o C to an optical density matching that of 0.5 McFarland turbidity
standard. This suspension was then used to inoculate Mueller Hinton agar
(MHA) plates by swabbing them with a sterile cotton swab. 30 µg discs of aztreonam, ceftazidime, ceftriaxone and cefotaxime were placed 15 mm (edge to edge) from an augmentin (amoxycillin-clavulanate; 20/10 µg) disc. Inoculated plates were incubated overnight at 37°C. Enhancement of the zone of inhibition between the clavulanate disc and any one of the β lactam
discs indicated the presence of an ESBL.[4],[6],[7]
Three dimentional tests (TDTs)
(i) Direct TDT
MHA plates were inoculated with test strains matching 0.5 McFarland
turbidity standard as described for DDS and a disc of ceftazidime, ceftriaxone,
cefotaxime or aztreonam was placed in the center of the plate. A well of
4 mm (diameter) was punched at a distance of 2 mm from the antibiotic disc.
The inoculum (30 µL) of the test strain in BHIB preadjusted to 5.0
McFarland standard was seeded into the well. Plates were then incubated
at 37°C for 24 hours. Heart shaped distortion of zone of inhibition with
growth of test organism appearing behind the well and reaching the well
was indicative of a positive TDT.[4]
(ii) Indirect TDT
MHA plates were seeded with the inoculum of a standard sensitive strain
( E. coli ATCC
25922) adjusted to McFarland 0.5 standard. A disc of ceftazidime, ceftriaxone,
cefotaxime or aztreonam was placed in the center of the plate. A well of
4 mm (diameter) was punched at a distance of 2 mm from the antibiotic disc.
The test strain (30 µL) in BHIB preadjusted to 5.0 McFarland standard, was seeded into the well. Plates were then incubated at 37°C for 24 hours. Heart shaped distortion of zone of inhibition around the β -lactam
disc as in the direct TDT was indicative of ESBL activity.[4]
Results
Among the 70 isolates of family Enterobacteriaceae analysed, eight isolates (4 E. coli , 3 Klebsiella spp. and 1 Enterobacter spp.)
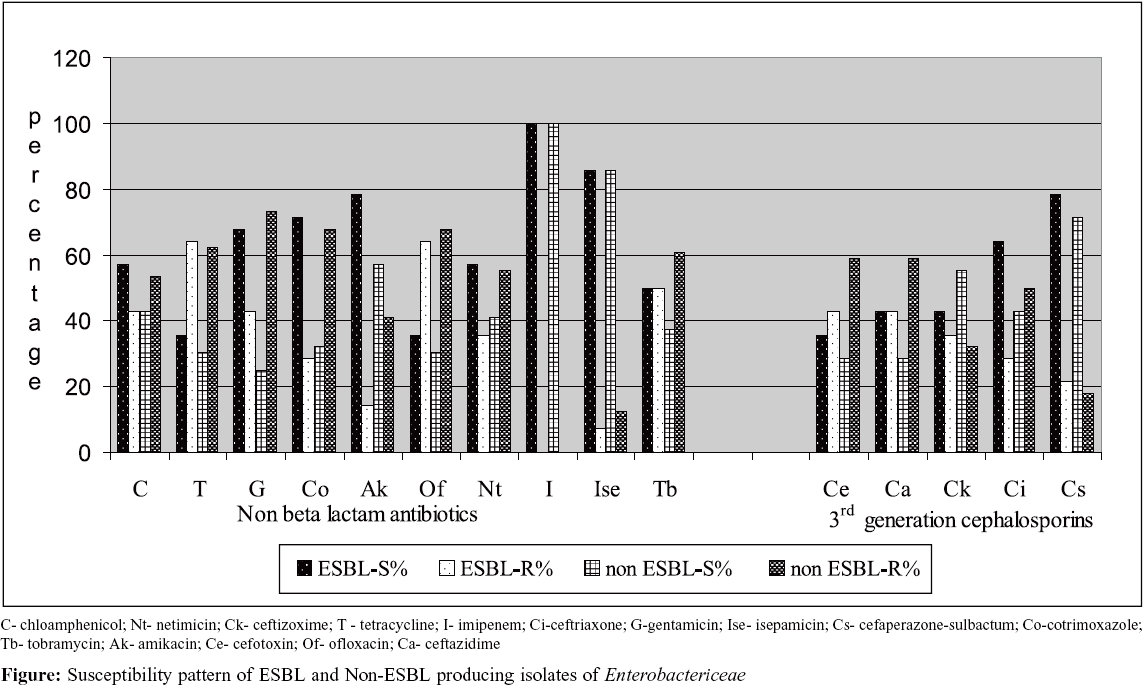
were susceptible to all antibiotics tested. Fifty-six isolates (80%) were resistant to three or more antibiotics tested. The sensitivity was 100% with imipenem, 85.7% with isepamicin and 72.8% with cefaperazone-sulbactum. The resistance was 70% against cefazolin followed by 67.1% resistance against cefuroxime, ofloxacin and gentamicin. The isolates that were resistant or showed decreased susceptibility to all four 3GC were tested 14.28% and 30% of isolates showed resistance to three 3GC.
Of the 70 strains tested, 14 (20%) were found to be ESBL producers. Seven (21.2%)
were Klebsiella spp, five (19.2%) E. coli and two
(28.5%) were Enterobacter spp. None of the Citrobacter spp.
demonstrated ESBL activity. Antibiogram profile of ESBL producers revealed
susceptibility to imipenem and piperacillin-tazobactum to be 100% and against isepamicin, amikacin and cefaperazone-sulbactum to be 85.7, 78.6 and 78.6% respectively [Figure - 1].
Two of the ESBL producers were positive by DDS (14.2%) with ceftriaxone and aztreonam indicator disks detecting one ESBL each. Theses two ESBL producers were also detected by the indirect TDT. Twelve (85.7%)
were positive by the TDTs (7 - direct, 5- indirect TDT) with aztreonam
detecting nine, ceftriaxone and ceftazidime detecting six each and cefotaxime
detecting five ESBL producers.
Discussion
Antibiotic resistance surveillance has a central role among all strategies to manage the problem of antibiotic resistance. Since their first description in the mid 1970s, ESBLs have been isolated worldwide and form a major contributor of drug resistance in many genera of Entererobacteriaceae .
Previous studies from India have reported prevalence of ESBL producers
to be 6.6 to 68%.[9],[10],[11],[12],[13],[14],[15],[16],[17] ESBL
production (68%) was reported among gram negative bacteria from
a teriary care hospital by Mathur et al.[12] Tankhiwale et al reported
that 48.3% of urinary isolates tested were ESBL producers.[13] Jain et al reported
86.6% of Klebsiella spp, 73.4% of Enterobacter spp
and 63.6% of Escherichia coli strains from cases of neonatal
septicaemia to be ESBL producers.[14] In
South India, Subha et al[15] have
reported 6.6% ESBL prevalence among Klebsiella pneumoniae from
children, whereas Babypadmini et al[16] have
shown 40% and 41% ESBL positivity among K. pneumoniae and E. coli respectively
in their study cohort. Another study reported an incidence of 58.06% for
ESBL producing E. coli and 57.14% for ESBL producing Enterobacter spp.[17] The
occurrence of ESBL producers among the Enterobacteriaceae isolates
in the present study was 20% while 28.5% Enterobacter ,
21.2% Klebsiella and 19.2% E. coli were
found to elaborate ESBLs.
As indicated in many previous studies, the 100% imipenem sensitivity in the present study, advocates usage of carbapenem antibiotics as the therapeutic alternative in the wake of the increasing resistance rates observed with conventional β -lactam
and non b-lactam antibiotics.
In the present study, TDTs were found to be better than DDS in the
detection of ESBLs. The combined positivity of both the TDTs was 85.7% against the 14.2% by
the DDS. Vercauteren et al[7] observed
93% positivity by DDS whereas, 79% positivity was reported
by Thomson et al.[4] Datta et al, have
reported TDT to be more sensitive than DDS.[11] As
observed in the present study, use of only one disk combination might fail
to detect ESBL production resulting in under reporting of prevalence. Simultaneous
use of 3GC and aztreonam disks with an augmentin disk is recommended in
screening for ESBL-producing organisms.
The susceptibility data collected in the present study demonstrates
the high degree of resistance among the major members of Enterobacteriaceae .
Continued monitoring of their susceptibility pattern is necessary in
clinical settings to detect the true burden of antibiotic resistance
for proper
disease management.
References
| 1. | Chaudary U, Aggarwal R. Extended-spectrum β -lactamases (ESBL) - An emerging threat to clinical therapeutics. Indian J Med Microbiol 2004; 22 :75-80. Back to cited text no. 1 |
| 2. | Jacoby GA, Medeiros AA. More extended-spectrum β -lactamases. Antimicrob Agents Chemother 1991; 35 :1697-704. Back to cited text no. 2 |
| 3. | Spanu T, Luzzaro F, Perilli M, Anicosante G, Tonioto A, Fadda G, et al . Occurrence of extended-spectrum β -lactamases in members of the family Enterobacteriaceae in Italy: Implications for resistance to β -lactamases and other antimicrobial drugs. Antimicrob Agents Chemother 2002; 46 :196-202. Back to cited text no. 3 |
| 4. | Thomson KS, Sanders CC. Detection of Extended-spectrum β -lactamases in members of the family Enterobacteriaceae : Comparison of the double-disk and the three-dimensional tests. Antimicrob Agents Chemother 1992; 36 :1877-82. Back to cited text no. 4 |
| 5. | National Committee for Clinical Laboratory Standards (NCCLS). Performance standards for antimicrobial susceptibility testing: Twelfth informational supplement. M100 - S12, 2002. Back to cited text no. 5 |
| 6. | Coudron PE, Moland SE, Sanders CC. Occurrence and detection of Extended-spectrum β -lactamases in members of the family Enterobacteriaceae at a veterans medical center: Seek and you may find. J Clin Microbiol 1997; 35 ;2593-7. Back to cited text no. 6 |
| 7. | Vercauteren E, Descheemaeker P, Ieven M, Sanders CC, Goossens H. Comparison of screenng methods for detection of Extended-spectrum β -lactamases and their prevalence among blood isolates of Escherichia coli and Klebsiella spp. in a Belgian teaching hospital. J Clin Microbiol 1997; 35 :2191-7. Back to cited text no. 7 |
| 8. | Emery CL, Weymouth LA. Detection and clinical significance of Extended-spectrum β -lactamases in a teriary care medical center. J Clin Microbiol 1997; 35 :2061-7. Back to cited text no. 8 |
| 9. | Shukla I. Tiwari R, Agrawal M. Prevalence of extended-spectrum β -lactamase producing Klebsiella pneumoniae in a tertiary care hospital. Indian J Med Microbiol 2004; 22 :87-91. Back to cited text no. 9 |
| 10. | Sumeeta K, Neelam T, Meera S. Extended-spectrum β -lactamase producing gram negative bacteria in a tertiary care hospital. Indian J Med Res 2002; 115 :153-7. Back to cited text no. 10 |
| 11. | Datta P, Thakur A, Mishra B, Gupta V. Prevalence of clinical strains resistant to various β -lactams in a tertiary care hospital in India. Jpn J Infect Dis 2004; 57 :146-9. Back to cited text no. 11 |
| 12. | Mathur P, Tatman A, Das B, Dhawan B. Prevalence of extended beta lactamase producing gram negative bacteria in a tertiary care hospital. Indian J Med Res 2002; 115 :153-7. Back to cited text no. 12 |
| 13. | Tankhiwale SS, Jalgaonkar SV, Ahamad S, Hassani U. Evaluation of extended spectrum beta lactamase in urinary isolates. Indian J Med Res 2004; 120 :553-6. Back to cited text no. 13 |
| 14. | Jain A, Roy I, Gupta MK, Kumar M, Agarwal SK. Prevalence of Extended spectrum-β -lactamase producing gram negative bacteria in septicaemic neonates in a tertiary care hospital. J Med Microbiol 2003; 52 :421-5. Back to cited text no. 14 |
| 15. | Subha A, Ananthan S. Extended-spectrum β -lactamase (ESBL) mediated resistance to third generation cephalosporins among Klebsiella pneumoniae in Chennai. Indian J Med Microbiol 2002; 20 :92-5. Back to cited text no. 15 |
| 16. | Babypadmini S, Appalaraju B. Extended-spectrum β -lactamases in urinary isolates of Escherichia coli and Klebsiella pneumoniae - prevalence and susceptibility pattern in a tertiary care hospital. Indian J Med Microbiol 2004; 22 :172-4. Back to cited text no. 16 |
| 17. | Ananthakrishnan AN, Kanungo R, Kumar A, Badrinath S. Detection of extended spectrum β -lactamase producers among surgical wound infections and burn patients in JIPMER. Indian J Med Microbiol 2004; 18 :160-5. Back to cited text no. 17 |
Copyright 2006 - Indian Journal of Medical Microbiology
The following images related to this document are available:
Photo images
[mb06033f1.jpg]
|

{kind=link}