 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
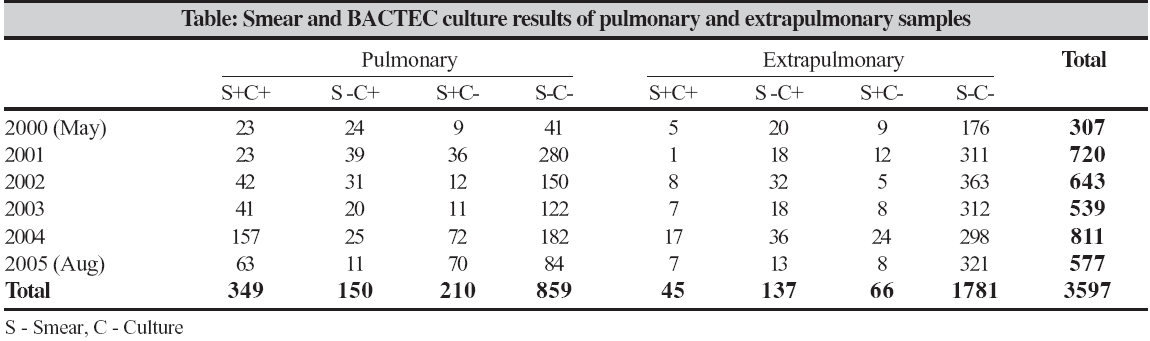
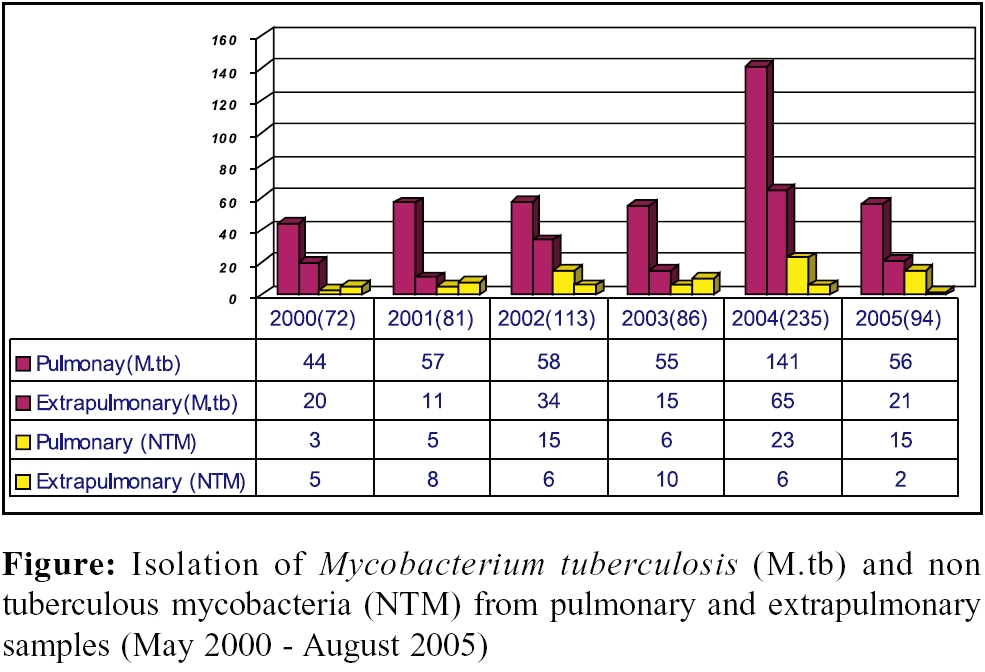
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 124-126 Brief Communications Isolation of mycobacteria by Bactec 460 TB system from clinical specimens *Lakshmi V, Patil MA, Subhadha K, Himabindu V Department of Microbiology, Nizam's Institute of Medical Sciences, Punjagutta, Hyderabad - 500 082, Andhra Pradesh Code Number: mb06035 Abstract This article reports our experience with the BACTEC 460 TB system in the past five years and its performance characteristics and its advantages over the conventional LJ medium for mycobacterial culture. Clinical specimens (3597) from patients suspected to have tuberculosis were submitted for mycobacterial culture between May 2000 and August 2005 and were processed using the BACTEC 460 TB system. Pulmonary samples were 1568 while the extra pulmonary samples were 2029. BACTEC achieved detection of 681 (18.93%) M. tuberculosis cases (499- pulmonary, 182- extrapulmonary) with a recovery time shorter by 13.2 days compared to conventional method, while 577 (84.7%) were non-tuberculosis mycobacteria. Automated systems can have a great impact and thrust on an early diagnosis of tuberculosis allowing an early and appropriate management of the patient and thereby a better disease outcome.Keywords: Mycobacteria, automated, BACTEC multidrug resistance Tuberculosis (TB) is a disease that physicians have recognized and grappled with through the millennia. The memorable and epoch making discovery of the Tubercle bacillus ( Mycobacterium tuberculosis, M. tb ) by Robert Koch in 1882 established TB as an infectious disease.[1] TB is still the first cause of disease due to a single infectious agent. Despite the availability of effective anti TB drugs, it continues to be a scourge for mankind. In association with the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS), TB is now considered a global threat.[1] Clinicians, as well as laboratory personnel, clearly realize the need for rapid detection and isolation of M. tb from the clinical specimen, including its differentiation from environmental Mycobacteria and the drug susceptibility of the isolates. This information is useful for initiation of timely and appropriate therapy in the patient. The emergence of multidrug resistant TB (MDR TB) in the present era of the HIV/ AIDS epidemic, further intensifies this need.[2] Bacteriological examination of the clinical specimens plays an important role in the diagnosis of any mycobacterial infection, more so for TB. The widely used acid fast smear (Ziehl Neelsen, ZN stain) for the demonstration of the acid fast mycobacteria, though rapid and simple to perform, has a low sensitivity, especially for single specimen and paucibacillary specimen. Also, it cannot differentiate live bacilli from inactive or dead bacilli.[3] A definitive diagnosis of active mycobacterial infection therefore depends on the isolation and identification of mycobacteria from the clinical specimen, by culture.[2] Traditional or conventional methods for mycobacterial culture utilize media containing egg or potato base (Middlebrook 7H10 or 7H11) or albumin (Lowenstein Jensen′s medium, LJ). While these media support the growth of mycobacteria, several weeks (2-8 weeks) of incubation may be necessary before the growth can be detected. This duration may further be prolonged in case of paucibacillary specimen. Also, an equal number of days may be required further to differentiate M. tb from non tuberculosis mycobacteria (NTM) and to test for the susceptibility of the isolate to anti TB therapy (ATT). Thus a considerable amount of time would be lost before the patient is put on proper ATT. Lack of standardization in methodology among laboratories, is another major limitation of the conventional methods.[3] There is thus a definite need for alternative culture methods that would rapidly detect and identify mycobacteria, including their drug susceptibility patterns, from clinical specimens.[3] The introduction of broth based growth systems, has significantly reduced the time to detection and increased the total number of positive cultures. The first such system developed was the BACTEC 460 TB system by M/s. Becton Dickinson, Cockins ville, Maryland USA.[4] Developed nations across the globe have used the BACTEC 460 TB as a routine method for mycobacterial isolation. However, there are very few centers in India which have adopted this system and are using it regularly on clinical specimen. This article reports our experience with the BACTEC 460 TB system in the past 5 years (2000 May-2005 August) and its performance characteristics and advantages over the conventional LJ medium for mycobacterial culture. Materials and Methods Three thousand five hundred and ninety-seven clinical specimens from patients suspected to have TB were submitted for mycobacterial culture between May 2000 and August 2005 (5 years). There were 1568 pulmonary samples while 2029 were extra pulmonary samples. The pus specimens were aspirates from deep-seated abscesses with features suggestive of a tuberculous abscess. The tissue specimens included biopsies from the ileocaecal mucosa, intracranial lesions and bone-lesions. All specimens were examined microscopically using the ZN stain for the presence of acid fast bacilli as per the standard protocol.[5] All the processed clinical specimens, both directly and after digestion and decontamination, were inoculated onto the LJ medium slopes and into BACTEC 12 B vial, Becton Dickinson.[4] The LJ medium slopes were prepared in-house[5] using dehydrated media from Hi-media (Mumbai) and fresh hen′s eggs. The quality of every batch of the medium was determined by its ability to support the growth of H37RV, a standard strain of M. tb . The medium used in the BACTEC 460 Tb system was 4 mL of Middlebrook 7 H12 broth with carbon 14 ( 14C) labeled palmitic acid. The clinical specimen was inoculated along with an antibiotic mixture containing solution - PANTA.[4] All the inoculated bottles were incubated at 37°C and observed for growth. LJ medium was observed on every alternate day for first week and once every week there after for eight weeks.[5] BACTEC 12 B bottles were read every alternate day for first week, the ninth and twelveth day and there after weekly once up to six weeks using the BACTEC 460 instrument.[4] The time to detection and total number of positive cultures recovered by both the methods were recorded. All the mycobacterial isolates from either of the culture media were differentiated by the NAP (para Nitro-a-acetyl amino-β -hydroxy propiophenone) test.[4] The average time for identification/differentiation between M. tb and NTM was four days. Results Significantly greater number ( P < 0.001) of mycobacteria could be isolated from the clinical specimen by the BACTEC (681/3597, 18.93%) than by the LJ medium (140/3597, 3.89%) The number and isolation rates from smear positive and smear negative pulmonary and extrapulmonary samples over the 5 years of the study are shown in the [Table - 1]. The recovery time of M. tb by the Bactec was shorter for smear positive specimens (pulmonary 3.2 days) than for smear negative specimens (pulmonary 15.9 days) while for extrapulmonary, smear positive or negative, it was same (21.8 days). The average recovery time on the LJ medium was four weeks for any type of sample. Differentiation of the isolates by the NAP test was done using the BACTEC system. Among the 681 mycobacterial isolates tested 577 (84.7%) were M. tb and 104 (15.3%) were NTM. Distribution of M. tb and NTM from pulmonary and extrapulmonary sources is shown in the [Figure - 1]. Discussion The widely used acid fast stain for the demonstration of the acid fast mycobacteria, though rapid and simple to perform, has a low sensitivity, especially for single and/ or paucibacillary specimen. Also it cannot differentiate live bacilli from inactive or dead bacilli.[2],[3] In 1969, Deland and Wangner developed a technique for automated detection of the metabolism of the bacteria by means of the 14sub CO 2 liberation during the decarboxylation of 14 C labelled substrates in the growth medium. Cummings and coworkers applied this principle to the detection of mycobacterial growth in 1975.[4] Middlebrook further improvised the technique and introduced 7H12 liquid medium with 14 C labelled substrate (BACTEC 12B) that is specific for mycobacterial growth.[4] The new radiometric medium significantly reduced the time taken for the primary isolation of mycobacteria from clinical specimen. Several studies have reported excellent recovery of mycobacteria from sputum and extrapulmonary specimens using an inoculum volume of 0.5 mL/4.0 mL of medium.[4] An antibiotic mixture, PANTA, (polymyxin B, amphotericin B, nalidixic acid, trimethoprim and azlocillin), is added to the 12B vial as a supplement to suppress the growth of contaminating organisms that may have survived the decontamination procedure during sample preparation. A growth promoting substance, polyoxyethylene stearate (POES) added to the 12B vial, enhances the growth of poorly growing M. tb strains. This substance is used in the PANTA reconstituting fluid required to reconstitute the lyophilized PANTA supplement.[4] Other studies have also shown similar time for recovery rates.[6],[7] Our study included samples from patients who were already on ATT. This would have a definite effect on the isolation rates. When only the samples from untreated patients are analyzed, the isolation rate increases to 26%. However, the automated system is very useful in the isolation of mycobacteria from smear positive extrapulmonary samples and smear negative samples. Clinically and epidemiologically, early differentiation of the M. tb from the NTM is more important than a complete speciation of the isolate. As the institution of ATT depends on the identification of the isolate, differentiation of the isolate as M. tb from NTM will help the physician in the appropriate management of the patient in a timely fashion. This is especially important in patients with HIV/AIDS, where there is clearly a need for the rapid differentiation of M. tb complex from the M. avium intracellulare complex.[2] The conventional methods used for differentiation are growth dependent and are hence slow, taking more than 2-4 weeks.[4],[5] The BACTEC NAP test uses an intermediate compound in the synthesis of chloramphenicol, which inhibits the growth of M. tb complex while the NTM are not inhibited. Average reporting time for the NAP test results is about four days. A definitive speciation of the isolate, if necessary, is by the conventional biochemical test procedure using growth on the LJ slants.[8] In conclusion, the ability of the BACTEC 460 TB system to rapidly detect mycobacteria from smear negative cases, especially in areas of high prevalence of TB, has definitely revolutionized the microbiological diagnosis of TB. As per our results, there was a definite reduction of time (about 2 weeks) in the time to detection by the BACTEC 460 TB as compared to the conventional method in smear positive specimens. The introduction of broth based growth systems, along with automation, like the BACTEC 460 TB system, have significantly reduced the time to detection and increased the isolation rates of mycobacteria from clinical specimens. The only constraint with the BACTEC is the cost, both initial and recurring and the need for a specialized setting. However, these limitations can be partially offset by the advantages of ease and early availability of reliable results by the system, especially in paucibacillary and extra pulmonary forms of TB. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06035f1.jpg] [mb06035t1.jpg] |
| |||||||||
{kind=link}
{kind=link}