 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
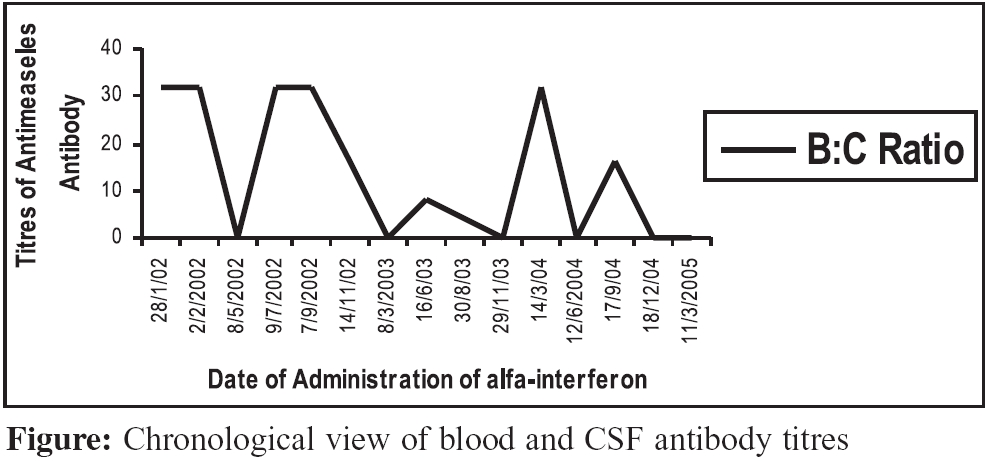
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 131-132 Case Report Role of CSF serology in follow-up of subacute Sclerosing Panencephalitis patients on treatment Gupta E, Dar L, Singh S, Behari M, *Broor S Depatment of Microbiology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029 Code Number: mb06037 Abstract Subacute sclerosing panencephalitis (SSPE) is a progressive inflammatory disease of the central nervous system with poor prognosis and high mortality. No effective treatment has a proven role; oral isoprinosine and intrathecal administration of a-interferon may prolong survival. We report an unusual case of adult onset SSPE patient on treatment with significant clinical improvement, even in the absence of conversion to seronegativity in either CSF or serum, on follow-up serological examination.Keywords: Subacute sclerosing panencephalitis, CSF serology, follow up. Subacute sclerosing panencephalitis (SSPE) is a progressive inflammatory disease of the central nervous system caused by a persistent, aberrant measles virus infection. In India, the incidence rate is very high (21 per million population), because of a higher proportion of measles cases in the very young, more frequent subclinical measles virus infection and perhaps due to a higher proportion of the total population below two years of age.[1],[2] The clinical course in SSPE is slowly progressive with death occurring within three years. Up to 10% of cases show either a fulminant or prolonged course.[2] The diagnosis of SSPE requires the fulfilment of at least three of the five criteria,[3] which include i) a typical clinical picture of progressive subacute mental deterioration with typical signs like myoclonus; ii) characteristic EEG changes; iii) elevated CSF globulin levels greater than 20% of total CSF protein; iv) raised titers of measles antibodies in blood and CSF and v) typical histopathological finding in brain biopsy or autopsy. Although no treatment has a proven effective role, oral isoprinosine and intrathecal administration of a-interferon may prolong survival.[4],[5],[6] In SSPE, specific measles virus antibodies are found in the CSF due to intrathecal production of antibodies as specific immune response to virus in the central nervous system (CNS). Presence of these specific antibodies helps in diagnosis as well as in follow-up of patient on treatment to assess improvement.[2],[7],[8] We report a case of adult onset SSPE patient on treatment with significant clinical improvement, even in the absence of conversion to seronegativity in either CSF or serum. Case Report A previously healthy 22 year old female presented to the Neurology Department at All India Institute of Medical Sciences (AIIMS), New Delhi, India, with history of myoclonus, cognitive disorder and visual disturbances for the past four months. Patient was unable to write, lost her memory and was unable to focus on reading. Patient had a history of measles infection in the childhood. Her developmental miles stones were normal. Family history was not significant. Specimen of blood and CSF were sent to the virology laboratory for anti-measles antibody titre estimation. Anti measles antibody titre was positive in both the CSF (1:4) and blood (1:128) samples by complement fixation test (CFT). Blood and CSF anti-measles antibody titre ratio was 32:1. EEG results demonstrated higher amplitude slow and sharp waves that recurred at interval of three seconds on a slow background, which supported the diagnosis SSPE. Based on three criteria- clinical presentation, EEG and laboratory findings, a diagnosis of SSPE was made. Patient was started with oral isoprinosine (500 mg QID) and intrathecal interferon - a-IFN (6 million units/dose). After three years of specific therapy patient′s condition improved substantially. Her vision improved, memory regained and she was able to write. She became independent to carry out her daily activities. Regular follow-up CSF and blood samples were taken from the patient for CSF and serum anti-measles antibody titre estimation. CSF and serum antibody titres showed rise and fall during the entire course and undetectable at times but never on a sustained basis [Figure - 1]. Discussion The pathophysiology of natural remissions and relapses in SSPE is unknown. The stable state may depend on a balance between viral replication and the body′s immune response. The CSF interferon levels are found to be low in patients with SSPE; exogenous administration of interferons possibly suppresses viral replication and augments the immune system of the body. CSF measles antibody titre estimation is considered quite effective along with EEG for assessing improvement in SSPE patient on treatment. The laboratory end-point of the treatment is the total eradication of detectable measles antibody from CSF.[7],[8] However, in our case, despite, specific treatment for three years and significant clinical improvement, no change in CSF antibody titre was seen. This case highlights that total eradication of antibodies in CSF may not occur and CSF antibodies may continue to persist for a long time. This may be due to the fact that virus is never really eradicated despite the available antiviral treatment. However, these observations need further evaluation and role of CSF serology in follow-ups of and SSPE patients on treatment needs to be defined. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06037f1.jpg] |
| |||||||||
{kind=link}