 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
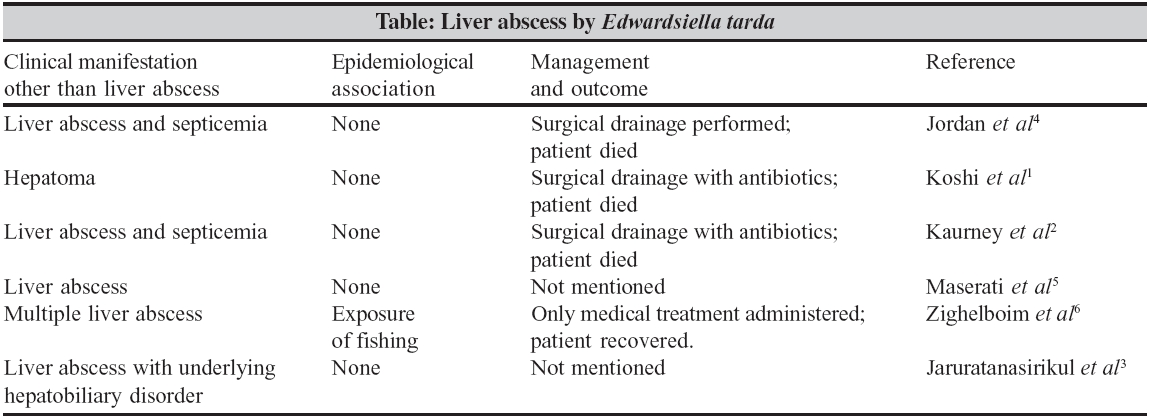
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 135-137 Case Report Liver abscess caused by Edwardsiella tarda biogroup 1 and identification of its epidemiological triad by ribotyping *Manchanda V, Singh NP, Eideh HK, Shamweel A, Thukral SS Department of Microbiology, University College of Medical Sciences and Guru Tegh Bahadur Hospital, Delhi - 110 095 Code Number: mb06039 Abstract Two clinical isolates and an environmental isolate of Edwardsiella tarda biogroup 1 (ETB1), recovered from liver pus, the stool specimen and from the pond water of the village of the patient, diagnosed to have liver abscess, were found to be identical by protein fingerprinting and ribotyping. It can be construed that the pond water served as the source of infection. The epidemiological triad of the agent (ETB1), host (the patient) and environment (pond water) was thus established. This is the first report in which the triad for extraintestinal Edwardsiellosis caused by ETB1 has been identified. This also constitutes the first report of typing of ETB1 strains by SDS-PAGE and ribotyping.Keywords: Liver, edwardsiella tarda, ribotyping, environment, liver abscess The three species of genus Edwardsiella , namely, E. tarda, E. ictaluri and E. hoshinae have a wide environmental distribution. Of these, E. tarda has been shown to be pathogenic in humans. It has been isolated from cold-blooded animals viz; cat fish, eels, amphibians and snakes with reptiles and marine fauna as its natural reservoirs.[1],[2] The disease spectrum resembles that of Salmonella infections.[3] This includes an asymptomatic carrier state, gastroenteritis and bacteremia.[2] Prevalence of carriage in stool is variable and is found to be higher in rural than the urban population.[1] The most common manifestation of E. tarda infection is diarrhoea. Extra intestinal manifestations have rarely been reported and include wound infections, bacteraemia, septicaemia, septic arthritis and liver abscess.[1],[4] Till date, six cases of liver abscess caused by E. tarda have been reported. [1],[2],[3],[4],[5],[6] A distinct biochemical variety generally referred to as ′ E. tarda biogroup 1′ (ETB1) that differs from the typical E. tarda strains in its inability to produce H 2 S on TSI agar and its ability to ferment sucrose, arabinose and mannitol, has been identified. The present study documents a case of liver abscess caused by ETB1. The two epidemiologic typing techniques viz; SDS-PAGE whole cell protein profiling and ribotyping were used to establish the source of extra intestinal infection caused by ETB1. Case Report A 26-year-old male presented with fever, chills and rigors since 15 days and complaints of pain in right hypochondrium. Physical examination revealed that the patient was in great distress and immobile because of pain. Patient was experiencing intermittent vomiting and was feeling anorectic for two days before reporting to the hospital. There was no history of jaundice or trauma, cough, diarrhoea and any episode of febrile illness in the recent past. He was a non-smoker and had never consumed alcohol. No immunization for hepatitis B was reported. Patient and his family had no history of tuberculosis or any other febrile illness. He was febrile with a temperature of 102oF, pulse rate was 110/minute, blood pressure was 120/70 mm of Hg and had a respiratory rate of 28/minute. There was no pallor, icterus, cyanosis, or peripheral lymphadenopathy. On examination of chest, intercostal tenderness was present below the right fifth rib. Chest was bilaterally clear with normal heart sounds. Per abdominal examination revealed soft abdomen with no liver and spleen palpable. Thumping sign was positive on right side. Haematological examination revealed haemoglobin to be 12.5 gm/dL, total leukocyte count 17,200 × 10 9 /L with differential leukocyte count of 90% neutrophils and 10% lymphocytes. ESR was raised to 110 mm after 1 hour. Random blood sugar was 112 mg/dl. Liver function tests were also normal with elevated serum alkaline phosphatase (SGOT - 37 KAU/100 mL and SGPT - 595 KAU/100 mL). Blood culture on three different occasions was sterile. Serological tests for Entamoeba histolytica and Echinococcus granulosus were negative. HIV serology was negative as determined by Tridot® ELISA assay. Chest radiogram revealed no abnormal findings. Ultrasound abdomen revealed an inhomogenous space-occupying lesion in postero superior quadrant of right lobe measuring approximately 8×8 cm in size. Diagnosis of liver abscess was made. Collecting bile ducts, gall bladder and portal vein appeared normal. Spleen and bilaterally kidneys revealed no abnormal findings. No free fluid was present in the abdomen. Pus aspirated by ultrasound guided FNAC was subjected to microbiological analysis. A gram stained smear of the pus aspirated from liver abscess showed few gram negative bacilli, large number of polymorphonuclear cells and necrotic debris. It was inoculated on blood agar and MacConkey′s agar plates and the culture grew Edwardsiella tarda biogroup 1.[7] The susceptibility of the isolate was tested by disc diffusion using Kirby-Bauer method and the results were interpreted as per NCCLS recommendations for enterobacteria.[8] ESBL production was detected using NCCLS standards. The patient′s stool samples collected on three consecutive days yielded growth of ETB1. He was started on chloramphenicol. Patient showed clinical improvement after 72 hours of starting the treatment. Patient was discharged on fourth day and he recovered completely by fifteenth day of follow up. A detailed history to determine the source of infection revealed that the patient was a strict vegetarian. He used to take bath in the village pond where he bathed his livestock also. There was no history suggestive of any kind of bite from aquatic fauna like fish or snake. He had no open wounds on his body and had no history of any injury in the recent past. The microbiological examination of the pond water was done using membrane filtration technique. Briefly, 500 mL of pond water was filtered through a Millipore filter (0.45 m pore size) and the membrane was placed on the surface of a MacConkey′s agar plate which was incubated at 37o C for overnight. The growth thus obtained was identified using standard procedures. The non-lactose fermenting colonies were identified as ETB1. The isolates were stocked as peptone agar stabs and stored at 4°C. The isolates from the three different sources had identical biochemical reactions and antimicrobial susceptibility patterns. The detailed antibiogram showed the isolates were sensitive to cephamycins (cefoxitin and cefotetan), amikacin, carbapenems (imipenem and meropenem), moxalactum, tobramycin, nalidixic acid, chloramphenicol and trimethoprim + sulphamethoxazole. The isolates were resistant to all cephalosporins including fourth generation except to those of cepham group, gentamicin, kanamycin, fluroquinolones, aztreonam and colistin. All the three isolates were found to produce ESBL. To determine the clonality of the isolates recovered from the three different sources, viz.; liver, stool and pond water, they were subjected to SDS-PAGE whole cell protein profiling. The whole cell protein samples from the three isolates were prepared using the method described by Costas et al , with few modifications.[9] The protein samples thus prepared were subjected to SDS-PAGE using the modified version of the technique of Laemmli.[10] Coomasie blue was used to stain the SDS-PAGE gel. The three isolates of ETB1 were subjected to ribotyping. The DNA from the bacterial strains was extracted using the method described by Boom et al and modified by Haertl et al , with minor modifications.[11],[12] Eco RI and pvu II enzymes were tried for digestion of extracted DNA. About 5 mg of the isolated DNA was completely digested with 20 U of pvu II but not by Eco RI in the reaction buffer supplied by the manufacturer (New England Biolabs, USA). Hybrids on the nylon membrane were detected by an enzyme immunoassay using alkaline phosphatase-conjugated anti-digoxigenin antibodies and color substrate mixture of nitroblue tetrazolium (NBT) and 5-bromo-4-chloro-3-indolyl phosphate (BCIP) substrates. Computerized numerical analysis of ribotyping and protein patterns was performed using the Diversity Database ® software version 1.1 incorporated into the gel documentation system (pdi, USA). Cluster analysis of the patterns was done using the unweighted - pair group method with arithmetic averages - UPGMA. All the three isolates were shown to belong to the same clone, both by protein profile analysis and ribotyping. The Pvu II ribopatterns had better resolved DNA bands than the ribopatterns generated by using Eco RI. Discussion E. tarda is an uncommon pathogen in humans. Infections in pediatric age group are primarily associated with gastrointestinal disease but extraintestinal manifestations are more common in adults.[3] Only six cases of liver abscess caused by E. tarda have been reported in literature [Table - 1]. In all the cases of liver abscess the patients had a significant clinical history and the causative agent ( E. tarda ) was isolated from liver pus as well as from blood specimens. The blood cultures in our patient were sterile. In most of the cases of liver abscess reported so far either source of infection remained unknown or there was only history suggestive of a possible source of infection. However, a definitive relation between the suspected source and the infection was not established. In the present study, we were able to trace the possible complete epidemiological triad of agent-host-environment. The agent being ETB1 in an otherwise healthy human host who had been exposed to pond water, from which the agent (ETB1) was isolated. Various routes of transmission like, faeco-oral route, wound exposed to the aquatic environment and accidental bites from aquatic animals have been proposed.[1],[3] Faeco-oral transmission is the most probable route of infection in this patient as the organism was repeatedly isolated from the stool specimen of the patient. Interestingly, the patient did not have a history of diarrhoea in the recent past, though diarrhoea is the most common manifestation of E. tarda infection . It is possible that the patient may have suffered a mild bout of diarrhoea and he was not able to recall. Till date, pathogenic status of ETB1 remains unknown. This constitutes the first case ever of infection caused by E. tarda biogroup 1. Ribotyping of Edwardsiella tarda has been reported for the first time is this study. Pvu II showed better ribopatterns than Eco RI. The results of ribotyping and whole cell protein profiling were relevant to the epidemiological data available. Further studies need to be done to evaluate the virulence and pathogenicity of this biotype of E. tarda. Moreover, we had just three isolates of E. tarda biogroup 1. More studies are needed to confirm the typing techniques used by us. Edwardsiella species should be considered as a rare cause of liver abscess especially in patients with rural background or with history suggestive of exposure to aquatic environment. Increased association with various clinical presentations and increasing antimicrobial resistance suggests it to be an important emerging pathogen that needs active monitoring and surveillance. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06039t1.jpg] |
| |||||||||
{kind=link}