 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
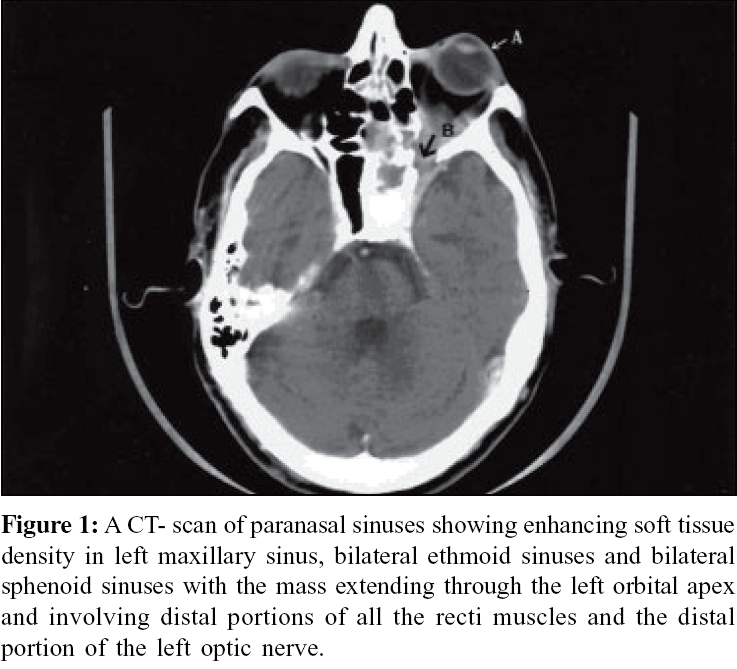
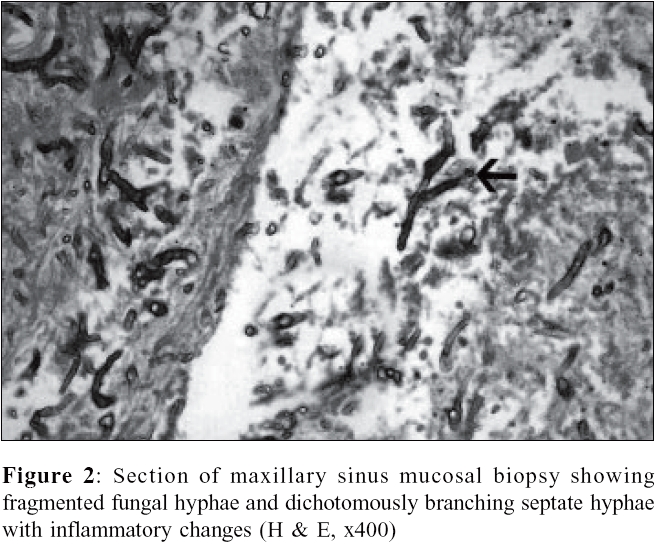
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 138-140 Case Report Sino-orbital Aspergillosis in a diabetic patient Sharada DM, Arunkumar G, Vandana KE, *Rao PS Department of Microbiology, Kasturba Medical College, Manipal - 576 104, Karnataka Code Number: mb06040 Abstract Sino-orbital aspergillosis in a 61-year-old male with uncontrolled non-insulin dependent diabetes mellitus presented with three months history of left ear pain, left side headache with mucopurulent nasal discharge and one week history of progressive swelling and pain with difficulty in opening of the left eye and sudden loss of vision. In spite of surgical debridement and medical management with amphotericin B and itraconazole his visual outcome was poor and the infection was unabated at one month follow up.Keywords: Aspergillosis, sinusitis, sino-orbital aspergillosis. Aspegillus sinusitis may be non-invasive or invasive. The non-invasive diseases include allergic sinusitis and Aspergillus fungal ball in sinuses. The invasive aspergillosis of sinus can be localized or fulminant.[1] Invasive Aspergillus infections are usually seen in patients with one or more predisposing factors such as neutrophil defects, corticosteroid therapy, human immunodeficiency virus infection, diabetes mellitus, alcoholism, prosthetic devices, trauma and advanced age.[2] Rare cases have been reported in immunocompetent individuals. Aspergillus fumigatus is the commonest species encountered in invasive aspergillosis.[2] The specific diagnosis of invasive sino-orbital aspergillosis is often delayed as it may mimic a number of infectious and inflammatory conditions like mucormycosis, malignancy etc.[2],[3] Response to treatment depends on early diagnosis and initiation of antifungal therapy augmented by surgical debridement. However, complete cure is rarely achieved.[2] Here, we report a case of localized invasive sino-orbital aspergillosis in an uncontrolled diabetes mellitus patient. Case Report A 61-year-old male with uncontrolled non-insulin dependent diabetes mellitus presented with three months history of left ear pain, left side headache with mucopurulent nasal discharge and one week history of progressive swelling and pain of left eye with difficulty in opening the eye. He had lost vision in left eye since three days. He was diabetic since five years and was not on any medication. Rhinoscopic examination revealed whitish crest over vestibules on both sides. All other ENT examinations were normal. Blindness in the left eye was confirmed by ophthalmologic examination. A CT- scan of paranasal sinuses [Figure - 1] showed enhancing soft tissue density in left maxillary sinus, bilateral ethmoid sinuses and bilateral sphenoid sinuses with the mass extending through the left orbital apex and involving distal portions of all the recti muscles and the distal portion of the left optic nerve. The mass was seen further extending into the adjacent brain parenchyma through the left superior orbital fissure. Right orbit and its contents were normal. In the light of CT findings differential diagnosis of mucormycosis or malignancy was considered. Biopsies were obtained from mucosa of nasal and sinus walls. The clinical and radiological diagnosis was mucormycosis was done involving left osteum, left anterior ethmoid, left posterior sphenoid and left maxillary mucosa and from the left middle meatus. Data of laboratory investigations were haemoglobin 13.6 gm/dL, packed cell volume 38.6%, total leukocyte count-14,900/cumm, platelet count 4,38,000/cumm, absolute eosinophil count 130/cumm; random blood glucose 490 mg/dL, fasting blood glucose 132 mg/dL, post prandial glucose 290 mg/dL, urea-45 mg/dL, creatinine-1.0 mg/dL, sodium -123 meq/L and potassium-4.2 meq/L. The patient tested negative for HIV antibodies and HBsAg by ELISA. Bacteriological culture of nasal discharge did not yield any bacteria. But fungal culture of the tissue from left maxillary sinus yielded Aspergillus fumigatus . Histopathological examination of the biopsy showed fragmented fungal hyphae and dichotomously branching septate hyphae with inflammatory changes [Figure - 2]. The patient was immediately taken for left functional endoscopic sinus surgery and debridement was done. He was started on amphotericin B and itraconazole. The patient responded well and was discharged. However, CT scan of PNS, microbiological and histopathological examinations revealed the persistence of the fungus in the affected sinuses at one month follow up. Discussion Invasive Aspergillus infections of the sinuses involving adjoining structures is a well documented cause of morbidity and mortality in immunocopromised hosts.[2],[3] There are many reports of invasive aspergillosis invading orbit and resulting in visual loss. However, early diagnosis of orbital involvement of fungal sinusitis continues to be a challenge. Localized invasive sino-orbital aspergillosis is a progressive, relentless and usually with fatal outcome. It is often seen in immunocompromised patients with one or more predisposing factors such as neutrophil defects, corticosteroid use, HIV infection, diabetes mellitus, alcoholism, prosthetic devices or trauma and advanced age.[1],[3] Nevertheless, it is occasionally reported in immunocompetent hosts.[2] The presentation of localized invasive sino-orbital aspergillosis can mimic infectious diseases such as mucormycosis, neoplastic, vascular and neuro-ophthalmic diseases.[2],[4],[5],[6],[7],[8] Specific diagnosis is essential for the appropriate clinical management of these patients. Our case presented with a four months history of left sided headache and left ear pain progressing to left eye swelling and pain before the sudden loss of vision. This is the typical clinical presentation of sino-orbital aspergillosis.[2] The CT findings were in concordance with previously published reports of sino-orbital aspergillosis. As in many other reports here also involvement of the sphenoid sinus was evident and the fungus invaded the orbit and optic nerve from the sphenoid sinus. The significance of this is that an early detection of involvement of sphenoid sinus could lead to an early clinical intervention preventing orbital invasion. However, a high index of clinical suspicion is required for this as the imaging findings may often be subtle. Steroid therapy worsens the course of fungal sinusitis therefore, it is necessary to rule out evidence of fungus by histopathological examination and culture of biopsies from the mass in sinuses. Often repeated biopsies are required to establish the involvement of fungus.[2] While CT or MRI of the paranasal sinuses can augment clinical suspicion, demonstration of the fungi in sinus mucosal biopsy may guide the management. But isolation of fungus from the sinus mucosal biopsy is the gold standard for the diagnosis of Aspergillus sinusitis.[2],[9] In the present case fungus was isolated in culture as well as demonstrated in the sections of biopsy confirming the CT and clinical findings of sino-orbital aspergillosis. Although our patient showed slight improvement after surgical debridement and medical treatment with amphotericin B and itraconozole, he continued to have Aspergillus in the sinuses as evident from the repeat histopathological examination and culture of sinus biopsy on his subsequent visit after one month of surgery. The uncontrolled diabetes and advanced age along with the invasion of the bone and possible invasion of the walls of the blood vessel affecting the poor penetration of drugs may be the reason for poor response in this case.[2] An early diagnosis and management of fungal sinusitis in this patient could have prevented the orbital involvement and loss of vision; however, our patient came for medical aid only at an advanced stage of the disease when he lost his vision. This is a common occurrence among patients with low socioeconomic status. Aspergillus sinusitis with orbital extension may often resemble mucormycosis and a variety of other inflammatory or neoplastic conditions. While imaging of the sinuses and adjoining structures provide complementary diagnostic evidence, demonstration of the fungi in tissue guides the treatment and isolation of the fungi confirms the diagnosis. Awareness of this disease and its clinical presentations may lead to earlier diagnosis and treatment which may increase the chance of better out come. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06040f1.jpg] [mb06040f2.jpg] |
| |||||||||
{kind=link}
{kind=link}