 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 144-145 Case Report Cyclosporiasis in an infant Iyer RN Department of Microbiology, Global Hospitals, Hyderabad
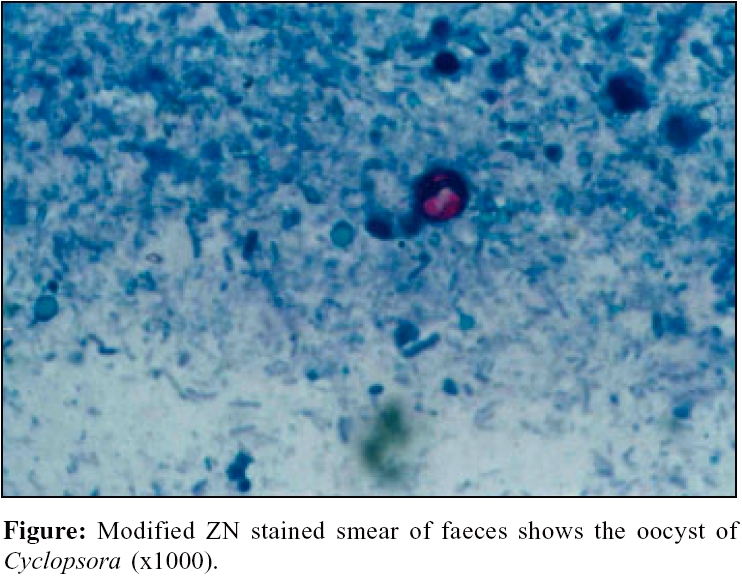
- 500 004, Andhra Pradesh Code Number: mb06042 Abstract This report describes cyclosporiasis in a seven month old infant who presented with incessant crying and refusal of feeds. The routine modified ZN stained smears showed the oocysts of Cyclospora when all other tests failed to reveal enteric pathogens. The need for the clinical laboratory to screen faeces samples for all possible pathogens in a given clinical situation needs to be emphasized.Keywords: Cyclospora, infant, faeces Acute diarrhoeal illness represents a significant health problem in children, particularly in infants where infective diarrhoeal disease can lead to suboptimal development. Whilst Cyclospora has been described in the literature as a cause of childhood diarrhea.[1],[2] there are no reports of an infant suffering from cyclosporiasis. The following case report is an attempt in this direction. Case Report A seven-month-old male infant, was brought to the out patient department with a history of low grade fever with incessant crying. The infant was feeding poorly over the past week. It was weaned off breast milk at the fifth month of life and was on artificial feeds including milk and infant solid feeds. The mother added that her child had an episode of diarrhoea with three loose stools, a day before the onset of symptoms. However, the baby did not have any previous episodes of vomiting or diarrhoea. On examination, the infant appeared ill at ease, was pale but not icteric. The infant was mildly febrile with a temperature of 99oF. A detailed examination of the cardiovascular and respiratory systems was unremarkable. An abdominal examination did not reveal any abnormality. Laboratory investigations included a complete blood count and ESR. The infant was also investigated for HIV infection and serum immunoglobulin levels were determined using rate nephelometry. Two faeces samples were collected for microbiological analysis and were processed in the laboratory within half hour of collection. The gross appearance of both samples was noted. Both samples were plated on blood agar, MacConkey′s agar, Sorbitol- MacConkey agar, Salmonella- Shigella agar, Hekton- Enteric agar, Wilson and Blair bismuth sulphite medium and selenite F broth medium which was subcultured on MacConkey′s agar after six hours of incubation at 37o C. Rotavirus antigen was tested using a sandwich ELISA technique. Parasitology studies were carried out on both the samples employing saline and Lugol′s iodine mounts, formalin ether concentration technique with wet mounts for examination and smears from the deposit for modified Ziehl Neelsen. Four smears were also made directly from both the faecal samples for a modified ZN stain(cold carbol fuchsin and with 3% acid alcohol) for the oocysts of coccidian parasites. A Sheather′s sucrose floatation technique[3] was carried out on both the samples to detect oocysts of Cryptosporidium species. Serotyping was done on E. coli isolates identified by biochemical reactions from the growth on MacConkey′s agar plates in an attempt to identify one of the strains of diarrhoegenic E. coli using standard antisera (BioRad). The haematological parameters were within normal limits. The HIV test was non reactive and the serum immunoglobulins were within normal limits. The faeces samples appeared mushy and ill formed with no obvious mucoid, purulent or bloody areas. Cultures did not reveal any pathogens. The Rotavirus antigen assay was negative in both the faeces samples. Saline and iodine mounts from both the faeces samples did not reveal any cysts or trophozoites of parasites. Sheather′s sucrose floatation technique did not reveal any oocysts of Cryptosporidium species. Modified ZN stained smears showed the oocysts of Cyclospora species (10-12 oocycts were seen in the entire smear). They measured 10-12 μ in size with variable staining characteristics that are typical of Cyclospora [Figure - 1]. A diagnosis of Cyclospora infection was made. The patient was treated with cotrimaxozole for seven days. Repeat faeces examination on follow up after two weeks and four weeks of initiating therapy did not reveal any oocysts of Cyclospora species. Discussion Cyclosporiasis is an emerging human disease, first described in humans in Papua New Guinea in 1977.[4] It is increasingly being identified in modified ZN stained smears of faeces samples from immunocompetent children, even in those with no history of travel.[5] Whilst cyclosporiasis has been reported in children, the exact prevalence of the infection in immunocompetent children in developing nations is not determined. Studies from Nepa and Peru have placed the highest incidence of infection in children aged 18 months to five years and the incidence is found to decrease with age.[6],[7] Infants who have been weaned off breast milk and given artificial feeds are at a risk for water borne cyclosporiasis. The present case is an example which also shows that not all cases of cyclosoriasis in infants will present with a watery diarrhoea. We believe that a single episode of loose stools with a low grade fever and incessant crying with refusal to feed may well be the presenting symptoms of cyclosporiasis. The diagnosis rests on the demonstration of the oocysts of cyclospora with their variable staining characteristics. It is also important to examine a modified ZN stained smear from the concentrated deposit of the faecal sample for these coccidian parasites as they would be missed if this exercise is not undertaken as in the present case. Special stains for coccidian parasites may be required to be performed on all faecal samples submitted for a diarrhoeal work up in the laboratory. Sole reliance on wet mount examination can lead to errors in identification of these parasites, particularly by inexperienced personnel.[8] Sporulation assays and molecular identification methods, though superior, are tedious, cumbersome and not available in al clinical laboratories. Cyclosporiasis should not be missed on a faecal prasitology examination as it is readily amenable to therapy with cotrimaxozole and a follow-up through faecal parasitology examination is possible. This also obviates unnecessary antibiotic therapy in children which only serves to augment antibiotic resistance. Hence, it is mandatory for all clinical microbiology laboratories to attempt to screen for all possible pathogens in faeces, irrespective of the age or the clinical presentation or the request made by a clinician as this enhances chances of detecting a treatable pathogen. Acknowledgement The author wishes to thank Dr. A. Venkatalakshmi, consultant paediatrician and neonatologist from Rainbow Children′s Hospital, Hyderabad, for her help in providing the clinical details of the patient.References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06042f1.jpg] |
| |||||||||
{kind=link}