 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
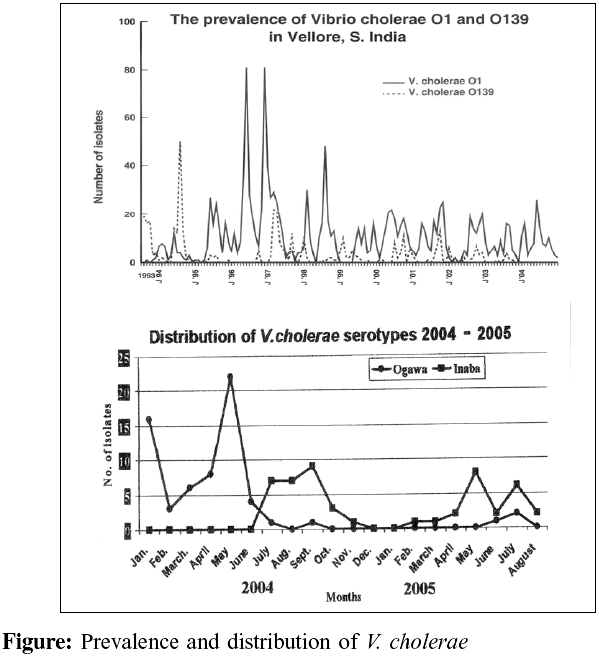
Indian Journal of Medical Microbiology, Vol. 24, No. 2, April-June, 2006, pp. 152-153 Correspondence Change in serotype and appearance of tetracycline resistance in V. cholerae O1 in Vellore, South India Jesudason MV Department of Clinical Microbiology, Christian Medical College, Vellore - 632 004, Tamil Nadu Code Number: mb06049 Dear Editor, We have been following various parameters in relation to the epidemiology of cholera in our area. We have monitored fluctuation among serogroups of V.cholerae .[1] We have looked at the environment as a possible reservoir and studied the effect of rainfall, temperature as possible factors influencing the epidemiology.[2] For the past two years, V. cholerae O1 is our predominant isolate [Figure - 1]. As far as the serotype is concerned, serotype Ogawa has been the common type we have been isolating, although routinely, each V. cholerae isolate is tested for agglutination with both Ogawa and Inaba high titer antisera. We have noticed a change in this pattern; serotype Inaba being more frequent currently. The observation which has caused concern is the appearance of tetracycline resistance in our strains. We have been carefully monitoring this and for the first time in three decades, we have eight such isolates (intermediate susceptible and resistant) since July 2005. The MIC of these strains ranges from 8 to16 μg/mL; ATCC S.aureus 29213 and E. coli 25922 were used as controls (MIC cut off for V. cholerae ; £ 4 susceptible, 8 intermediate and > 16 resistant). It is interesting to note that the tetracycline resistant strains are all of the Inaba serotype; the Ogawa strains are tetracycline sensitive. Could this be why the Inaba serotype has emerged as the predominant serotype? Norfloxacin is the preferred treatment of cholera these days and therefore our finding may not seem of importance in cholera treatment. It is, however, a land mark in our centre for these are the first isolates to show tetracycline resistance. We have already reported that our V. cholerae O1 show resistance to nalidixic acid and cotrimoxazole[3],[4] and this continues to be so for both Ogawa and Inaba strains. We continue the monitoring to see the trend. This may well be an indication of emergence of MDR strains in future. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06049f1.jpg] |
| |||||||||
{kind=link}