 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
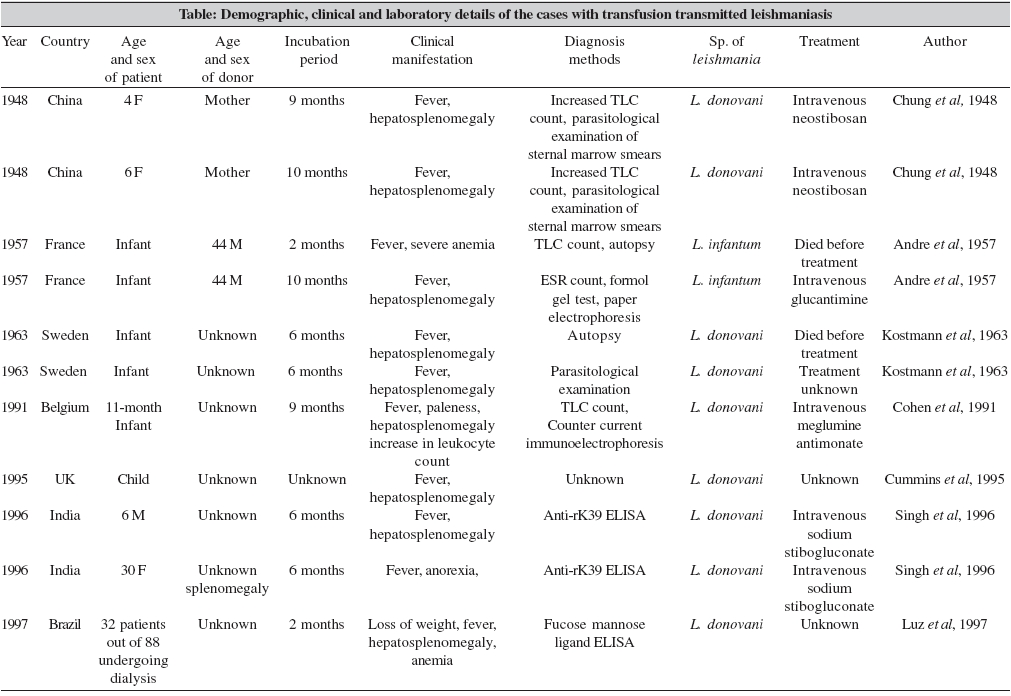
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 165-170 Review Article Transfusion transmitted leishmaniasis: A case report and review of literature Dey A, Singh S Department of Laboratory Medicine, All India Institute of Medical Sciences, New Delhi - 110 029 Code Number: mb06052 Abstract Leishmaniasis is caused by the infection of haemoparasite Leishmania . The disease is a major public health problem in at least 88 countries, including India. Various species of Leishmania are involved in causing this disease. In India, Leishmania donovani species causes visceral leishmaniasis or kala-azar. The parasite is mainly transmitted from infected to uninfected person through the bites of female sandfly. Rarely the parasite can transmit through placenta from mother to child, through sexual intercourse, as laboratory acquired and through blood transfusion. This paper reports a unique case of transfusion-transmitted fatal kala-azar in an Indian infant who acquired this infection within few days of his birth after receiving blood from his maternal uncle, who was asymptomatic at the time of blood donation but died due to severe kala-azar within three months. The baby started having fever and developed hepatosplenomegaly within one month of blood transfusion and in spite of repeated anti-leishmanial treatment with sodium antimony gluconate the child died at the age of 7 months. This paper details the clinico-pathological findings of this child and also reviews the literature on this aspect and its impact on transfusion medicine.Keywords: Blood bank, India, kala-azar, mode of transmission, transfusion-transmitted Leishmaniasis, a vector-borne parasitic disease, is caused by obligate intramacrophage protozoan. The parasite is characterized by diversity and complexity.[1],[2] The infection presents with a wide range of clinical forms.[3] The visceral leishmaniasis (VL), also known as kala-azar, is the most severe form of the disease, which, if untreated, has a mortality rate of almost 100%.[1],[2],[3] The cutaneous leishmaniasis (CL) produces skin ulcers on the exposed parts of the body, such as the face, arms and legs. The number of ulcers may vary from one to as many as 200, causing serious disability and leaving the patient permanently scarred. The third form is mucocutaneous leishmaniasis (MCL) or espundia. It can lead to extensive and disfiguring destruction of mucous membranes of the nose, mouth and throat cavities and can involve even the cartilages. Sometimes the cutaneous form may lead to disseminated form, known as diffuse cutaneous leishmaniasis (DCL).[2] Leishmaniasis is a public health problem in at least 88 countries, of which 67 are in the old world and 21 in the new world.[2] The countries from all the four major continents - Africa, South America, Asia and Europe are affected with this infection. More than 90 percent of visceral cases appear in India, Nepal, Bangladesh, Sudan and Brazil.[2],[3],[4] Similarly, about 90% of all cases of mucocutaneous leishmaniasis (MCL) occur in Bolivia, Brazil and Peru and 90% cases of cutaneous leishmaniasis (CL) occur in Afghanistan, Brazil, Peru, Iran, Saudi Arabia and Syria. About 1-1.5 million new cases are reported annually worldwide.[2] The geographical distribution of leishmaniasis is limited by the distribution of the sand fly, the main vector of this disease. Leishmaniasis is transmitted by about 30 species of Phlebotomine sandflies, which is the commonest mode of transmission. It is presumed that skin lesions or peripheral parasitaemia act as reservoirs, from where the female sandfly takes up the infective form of the parasite (amastigotes) during the blood meals and transmits to new human host through another bite. Other than the insect route, transmission through placental,[5] semen,[6] injection needles[7] and laboratory acquired[8] infections have also been reported, though rarely. However, much attention has been invited on preventable and iatrogenic causes of leishmaniasis that include transfusion-transmitted route.[9],[10],[11],[12],[13],[14] The American Association of Blood Banks has recommended ban on blood donations from a select group to prevent transfusion transmitted leishmaniasis (TTL).[15],[16] We have earlier reported three cases of TTL from India.[13] In this paper we report an unique fatal case of TTL in an infant whose source was none other than his maternal uncle. Here, we also review the literature for clinical and other details of transfusion-transmitted leishmaniasis and its impact on transfusion medicine. Case Report A 7-month-old child from kala-azar endemic district of Samastipur, Bihar, was brought to the All India Institute of Medical Sciences, New Delhi in September 2003, for pallor, fever and abdominal distension off and on since first month of life. He was hospitalized on 6th September, 2003. On examination he was found severely anaemic with respiratory distress. His spleen was 13 cm enlarged and liver was soft but 11 cm below right costal margins. The maternal history revealed that the baby was born as full term through lower cessarian section route and owing to severe paleness he was given 1 unit (100 ml) of whole blood on day 7 of life locally in Bihar. The blood donor was his maternal uncle, who was healthy and asymptomatic at the time of donation but died at the All India Institute of Medical Sciences, New Delhi, within 3 months due to hepatosplenomegaly with pyrexia of unknown origin. The diagnosis of visceral leishmaniasis could be established only on post-mortem examination. The child was referred to All India Institute of Medical Sciences with no improvement in paleness. Two months before referring to this hospital, the local physicians in Bihar had investigated him for Kala-azar and found splenic aspirate and bone marrow smears positive for Leishman-Donovan (LD) bodies and he was given antileishmanial treatment in the form of injections (records not available), but without any clinical improvement. His family history revealed that the boy was youngest of the four siblings, the eldest being 13 years. All three siblings were alive and healthy. At the All India Institute of Medical Sciences, differential diagnoses of chronic myeloid leukemia and metabolic disorder disease were made along with kala-azar. The repeat bone marrow aspirate examination did not reveal any finding suggestive of haematological or metabolic disorder nor any LD bodies were seen. However, his bone marrow biopsy on 8th September, 2003 showed haematopoietic cells of all series with increased plasma cells and lymphocytes and the biopsy was positive for LD bodies. There was also grade 1 myelofibrosis. His liver biopsy done on 15th September, 2003, revealed findings compatible with steatohepatitis, with fatty macrovesicular changes with numerous spotty necroses with small lipid granuloma. Apoptotic hepatocytes and occasional giant cells and focal areas of pericellular fibrosis were also identified. During his hospital stay his routine laboratory investigations revealed a haemoglobin values between 7-9 gm%, total leukocyte count between 3000-5000/cmm and raised liver enzymes. His blood samples were also sent for antileishmania (rK-39) antibodies. For antileishmania antibody detection in-house enzyme linked immuno sorbent assay for anti-rK39 IgM and commercially available rapid test (InBios ®, USA) were performed in our laboratory as published elsewhere.[17] This antibody detection is reported to be 100% specific for kala-azar diagnosis.[18] Both these tests were found to be highly positive for antileishmania (rK-39) antibodies. However, his mother and other family members were found to be negative for antileishmania antibodies. After the diagnosis of leishmaniasis, sodium antimony gluconate (SAG, 20 mg/kg) was started on 18th September, 2003, intravenously, along with other antibiotics. Two units of whole blood were also given at this hospital during the hospitalization period. However, his fever persisted between 100-102o F. During the treatment period, he also developed septicaemia and multiple organisms ( Staphylococcus , Klebsiella and Pseudomonas), were grown from his blood culture. His serum bilirubin increased to 2.5 mg with increased OT/PT (178/82 I.U.). On 28th September, his SAG treatment was changed to amphotericin B (3 mg/ kg). On the same day his splenic aspiration was performed which was found to be diluted with blood and did not show any LD bodies nor any malignant cell. On next day of starting amphotericin B his total leucocytes count dropped to 1800/cmm and his condition deteriorated further. He developed bleeding through mouth, nose and intestine. He also developed pulmonary bleeding with severe respiratory distress and died after 2 days on October 1st, 2003. Review of Literature This case report indicates that transfusion transmitted leishmaniasis (TTL) continues to be a major problem in areas where kala-azar is endemic. It also poses a diagnostic problem as most of these cases manifest atypically. The present case was an example where the conventional methods including splenic and bone marrow aspirates failed to demonstrate LD bodies. The pre-existing myelofibrosis and possibly incomplete treatment further complicated the diagnosis. Whether the myelofibrosis in this patient was pre-existing before he got transfusion transmitted leishmaniasis or it developed due to leishmaniasis[19] can not be explained fully because bone marrow biopsy was not done locally before first blood transfusion was planned to ascertain the cause of pallor. Therefore, sensitive serological tests like anti-rK39 or anti-rKE16 antibodies[20] or bone marrow biopsy need to be done to clinch the diagnosis. In the present case the failure of SAG treatment to cure the infection is on expected line, because the patient came from Samastipur District of Bihar, where more than half of the kala-azar patients are SAG resistant. Whether this resistance was primary or developed after suboptimal treatment is uncertain. After HIV epidemic, most of the countries have adopted a policy of rational use of blood and safe blood transfusion. Despite this, a number of pathogens including viruses and parasites such as Plasmodium, Toxoplasma, Leishmania and Babesia continue to get transmitted through transfusion.[21],[22],[23],[24] This is expected since except screening for HIV, hepatitis B and C, majority of blood banks do not screen donor blood samples for other potentially pathogenic organisms, such as Toxoplasma and Leishmania . L. donovani are expected to remain present in the blood for an undefined period between the bite of sand fly and their final localization to the target organs. Several in vivo studies have proved that the parasite after entering the skin, invades the cells of the reticulo-endothelial system where it resides and multiplies.[20] The parasites can be found within large mononuclear cells and polymorphonuclear leukocytes and are expected to be present in the blood for an undefined period following the bites of sand flies.[1],[25] The development of disease starts with an asymptomatic subclinical period in which parasites may already be circulating in the peripheral blood, but without clinical or haematologic changes.[17],[26] These parasitaemic blood donors usually have a very low parasite density and serve as a source of transfusion transmitted leishmaniasis. Circulation of Leishmania donovani and L. tropica in the peripheral blood of asymptomatic individuals[27],[28] and circulation of Leishmania braziliensis in cured cases have been reported.[29],[30] The duration of asymptomatic parasitaemia varies with the infecting species. For Leishmania donovani this period varies from 1-14 months.[28] For other species this period varies from two to eight weeks, although some cases have been reported following a one-year incubation period. Usually asymptomatic infection does not persist for more than one year, but rarely asymptomatic infection may last for decades.[29] However, with the advances in diagnostic techniques such asymptomatic cases of leishmaniasis can be diagnosed comparatively easily. Recently in kala-azar endemic areas of India, a high percentage of such cases were reported.[17] Survival of Leishmania in blood and blood products Similar to in vivo findings, in vitro studies have clearly shown that viscerotropic L. tropica survived as intracellular parasites in monocytes for 30 days at 4oC and for at least five days at 24oC.[28] Intracellular parasites survived longer than did stationary phase extracelullar promastigotes or free amastigotes. The parasites survived as intracellular forms in monocytes for 25 days in the red blood cell fraction kept at 4°C, five days in the platelet fraction kept at 24°C, 35 days in the red blood cell fraction frozen with glycerol and for 30 days in unprocessed whole blood left at 4°C. Identical experiments with L. donovani resulted in comparable survival data. To define the minimum number of L. tropica needed to contaminate 1 ml of blood, serial dilutions with known numbers of intramonocytic amastigotes per milliliter of blood were cultured in whole blood at 4°C and aliquots removed every day to determine parasite viability. It was determined that one detectable viscerotropic L . tropica parasite survived for 15 days when whole blood was kept under blood bank conditions, but an inoculum of 256 organisms was required for a 35-days culture to have viable parasite(s).[28] Animal studies carried out to determine the presence of infected monocytes in the blood of cutaneously infected animals and the possibility of transmitting the disease by blood transfusion from both infected donor animals and seeded CPDA-1 bag of human whole blood kept for 30 days at 4°C under blood bank conditions. Viscerotropic L. tropica and cutaneous L. major were cultured from the blood of six of 10 (60%) cutaneously infected hamsters and from five of nine cutaneously infected BALB/C mice, respectively. Cutaneous lesions or metastasis to the lower extremities developed in three of the five mice transfused with a fresh 0.5 ml blood sample from lesion-positive BALB/C donor mice. In addition, L. major amastigotes were visualized and cultured from the liver and spleen of four of the five transfused animals. Similarly, four of the five mice transfused with blood stored at 4oC for 30 days showed metastasis to the face and upper extremities. Amastigotes were visualized and cultured from the livers of all five transfused animals. All three additional animals who received 0.25 ml of blood from a CPDA-1 bag seeded with 10[5] L. tropica amastigotes per mL of blood and stored for 30 days also developed metastasis to the lower extremities or face. Thus it was clearly proven that Leishmania not only survives under blood bank conditions, but the parasites retain their infectivity to healthy experimental animals.[28] Transfusion Transmitted Leishmaniasis We could find only 11 reports of transfusion-transmitted leishmaniasis in the English literature [Table - 1]. Of these, 10 were individual case reports and in one paper from Brazil 32 cases of kala-azar were reported out of 82 patients undergoing haemodialysis.[14] All 10 individual case reports were from Asia and Europe. Out of the 10 reports, five were infants and four patients were children of less then 6 years age. Only one adult case of transfusion-transmitted leishmaniasis was reported in a 30 year old female from Haryana, India.[13] The time between the transfusion of the Leishmania infected blood and first clinical manifestation was available in 10 reports; and the mean incubation period was 7.4 + 5 months. In all patients including the 32-dialysis patients, fever was the absolute symptom, present in all (100%) patients following hepatosplenomegaly (82%), isolated splenomegaly and severe anaemia (9% each). The antemortem parasitological laboratory diagnosis could be confirmed only in three children, while in two infants the diagnosis was made on autopsy examination. In two patients conventional serological methods were used to reach the diagnosis, while in two patients previously reported by us[13] and the case presented here, the diagnosis was made by anti-rK-39 antibody detection. It is interesting that all patients who could be offered treatment responded to stibogluconate, except the present case. The first report of transfusion-transmitted kala-azar came from China in 1948.[31] The blood was donated from infected mother to two daughters. One was four and another six year old. Intramuscular injection of 20 mL of mother′s blood was given to these daughters as a prophylaxis for measles prevention. After a few days the mother was admitted to a local hospital for paleness, fever and distension of abdomen and was diagnosed with kala-azar one month later. Both the daughters were closely observed and both developed kala-azar nine and ten month after receiving the transfusion, respectively.[31] Other reports of transfusion-transmitted kala-azar followed these two reports and have been reported from France,[9] Sweden,[10] Belgium,[11] United Kingdom,[12] India[13] and Brazil.[14] A 44-year-old French man donated blood to two newborn infants in September 1955 after traveling to Spain. He later developed skin rash and lymphadenopathy. The scraping from the skin nodules showed amastigotes. One blood recipient infant developed anaemia after 10 months, which progressed to kala-azar. The Leishmania infantum were grown from the bone marrow of this child. The other infant died within three months.[9] From Sweden, two cases of transfusion-transmitted kala-azar were reported.[10] Blood from a healthy asymptomatic donor who had been outside the country in recent years was given to these newborns. Both fell ill six months after receiving the transfusion. One newborn died and an autopsy revealed kala-azar. The second new born was treated and survived. In Belgium the first case of transfusional transmission leishmaniasis was reported in 1991 in a 11 month old infant who had never left his native country.[11] Shortly after the birth, the child was repeatedly transfused for anaemia just like our case. The period of incubation in this case also, like other cases reported from China and Spain, was 9 months. Case of transfusional leishmaniasis affecting a child has also been reported from United Kingdom.[12] An English child developed visceral leishmaniasis after cardiac surgery. Neither he nor his mother had ever been out of the UK and his disease was probably transmitted by blood transfusion. Several of these cases occurred more than 40 years ago when donor screening programmes were not that stringent. It was interesting to note from the literature that the majority of infected recipients were young children or neonates. Only from India one adult case of TTL was reported.[13] The case was from Haryana state of northern India, a non-endemic area. The patient had received blood transfusion for haemorrhagia. The patient had never visited any area endemic for L. donovani . In contrast, the case reported here is a child from endemic area for kala-azar where possibility of congenital transmission was also considered.[5] But this was ruled out by her mother′s sero negative status for leishmaniasis. No other family member was having kala-azar during the time of illness thus ruling out the possibility of vector borne acquisition of this parasite. Also on the basis of the sequence of events, incubation time and strong antibody reaction, we conclude that the case was a transfusion transmitted kala-azar. In India migration of residents from kala-azar endemic states to Delhi and other Western parts of India is a major issue. Unemployment is high among these migrants and some resort to selling their blood. The risk of transfusion-transmitted kala-azar may be worsened by the short supply of blood in Delhi. Due to huge gap in the demand and supply of the blood only a few units can be stored at 4oC for a period of 35 days which is required to kill this parasite under blood banking conditions.[28] Although no case of transfusion transmitted leishmaniasis has been reported from the United States, concern over the possibility of TTL was raised at the time of operation desert storm. On November 12, 1991, the department of defense informed the public of a newly recognized form of viscerotropic leishmaniasis due to L. tropica among military personnel and consequently American Association of Blood Banks (AABB) recommended that individuals who had traveled to or visited Saudi Arabia, Kuwait, Iraq, Oman, Yemen, Qatar, Bahrain or the United Arab Emirates on or after August 1, 1990, should be deferred as donors of transfusable blood components until January 1, 1993.[15] The American Association of Blood Banks, Arlington, suggested that TTL can be prevented by applying a blanket policy of not drawing blood from individuals who are at potential risk of being infected with the parasite.[16] The published data suggest that above policy needs reconsideration. As the impact of this on the blood supply is expected to be significant, although it is difficult to project the exact number of donors who will be deferred. Screening of Donor Blood Screening of donated blood by microscopic examination is not a sensitive tool and aspirates from the spleen or the bone marrow will be unethical. Immunodiagnostic testings, including ELISA using recombinant antigens such as rK-39 developed from Leishmania chagasi of the new world or a recently developed recombinant antigen rKE16 from Leishmania donovani from India[20],[32] and PCR technology can be used for mass screening of donor blood samples. But these methodologies may have financial and technical difficulties. It may be suggested that, all donors be screened for specific antileishmania antibodies. A rapid test using rKE16 antigen developed by us with the financial support from department of biotechnology is now commercially available at a very economic price.[20] Use of this may be feasible in India from where maximum cases of transfusion transmitted kala-azar are reported. However, some workers believe that universal screening for antileishmanial antibodies and discarding the blood of Leishmania -seropositive donors, would decrease the blood supply. Currently this remains a debatable issue. Studies appropriately designed to study the prevalence and cost-benefit ratio are needed to determine whether screening of donor blood for antileishmanial antibodies needs to become a routine procedure in blood banks.Acknowledgements The authors wish to thank Prof. LS Arya, Department of Paediatrics, All India Institute of Medical Sciences, New Delhi for providing clinical details. Technical assistance of Mrs. Veena Balooni is also acknowledged.References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06052t1.jpg] |
| |||||||||
{kind=link}