 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 171-176 Special Article Antifungal susceptibility testing method for resource constrained laboratories Khan S, Singhal S, Mathur T, Upadhyay DJ, Rattan A Department of Infectious Diseases, Ranbaxy Research Laboratories, Gurgaon - 122 001, Haryana Code Number: mb06053 Abstract Purpose: In resource-constrained laboratories of developing countries determination of antifungal susceptibility testing by NCCLS/CLSI method is not always feasible. We describe herein a simple yet comparable method for antifungal susceptibility testing. Keywords: Antifungal susceptibility testing, minimum inhibitory concentration, NCCLS/CLSI, semisolid agar Invasive fungal infections have not only increased in frequency but also new fungal species have been reported to cause infection, especially in immunocompromized patients. Concurrent with the increase in fungal infections, a large variety of antifungal drugs are available with different spectrum of activity. There is therefore a need to determine the antifungal susceptibility of isolates to available drugs. NCCLS (now clinical and laboratory standard institute, CLSI) has recommended methodologies to be used for yeasts[1] and filamentous fungi[2] susceptibility testing. These methodologies give reproducible results. E-test, Alamar Blue, ATB fungus, API, Vitek and Disc diffusion have emerged as alternative techniques to address issues in different laboratories. [3],[4],[5],[6],[7],[8] In each new methodology comparison has been made to MIC results obtained by NCCLS / CLSI methodology. NCCLS / CLSI gives reproducible results, however many of our colleagues from different part of India have expressed their inability to perform NCCLS / CLSI method for various reasons. One option is to collect the isolates and determine the MIC in a reference laboratory, but the inevitable delay involved would make the exercise only of academic interest. The other option is to develop a simple methodology and compare its performance with the NCCLS / CLSI methodology enabling resource-constrained laboratories to determine the antifungal susceptibility in clinically useful timeframe. To cater to the need of these resource-constrained laboratories it is important to have an antifungal susceptibility testing method which give results that correspond to the clinical outcome of antifungal treatment, show correlation to those obtained with the reference method as recommended by NCCLS / CLSI and be reproducible. The system would be more acceptable if it is rapid and easy to perform. The purpose of this study was to compare results of antifungal susceptibility testing of fungal isolates by NCCLS / CLSI broth microdilution and the semi solid agar antifungal susceptibility(SAAS)[8],[9],[10] method against antifungal agents: fluconazole (FCZ), itraconazole (ITZ), voriconazole (VCZ), amphotericin B (AMB), cancidas (CAN) and terbinafine (TER). Materials and Methods Organisms Antifungal agents Antifungal susceptibility testing Selection of suitable medium for SAAS method Preparation of drug supplemented tubes
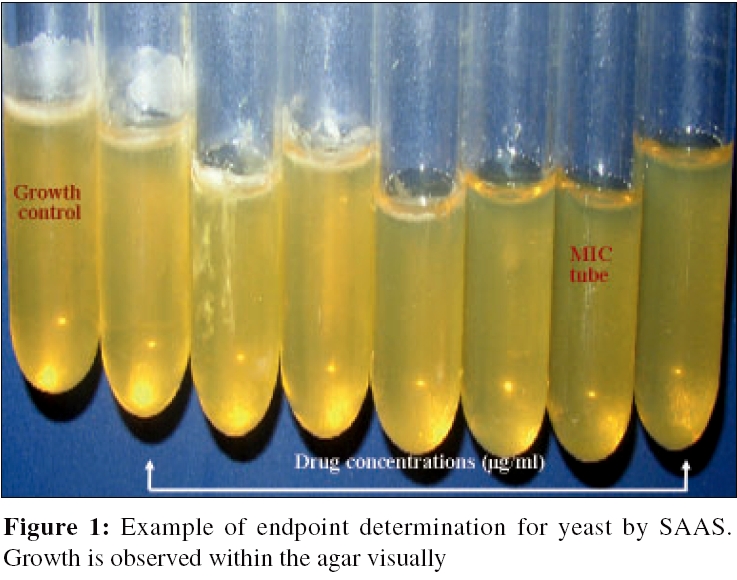
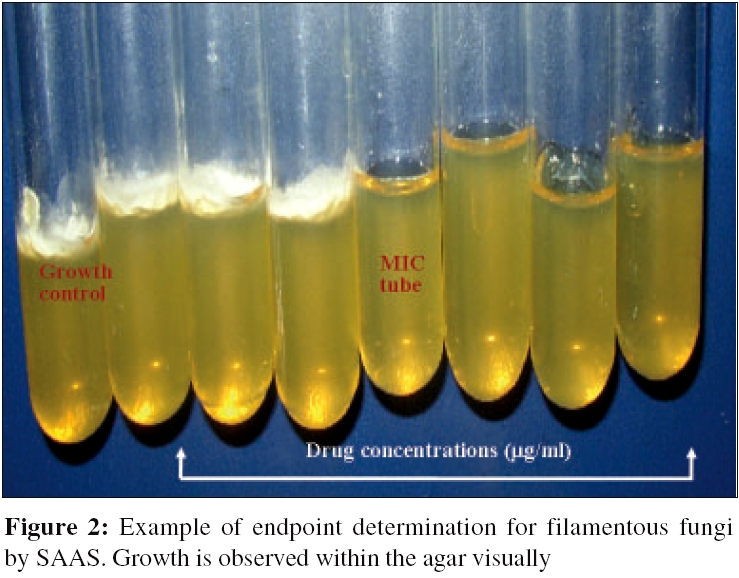
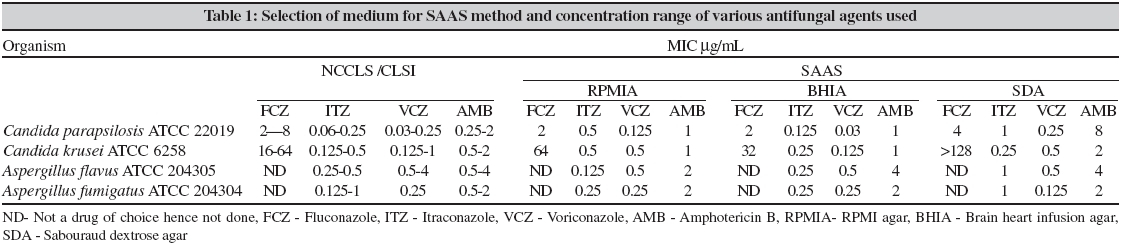
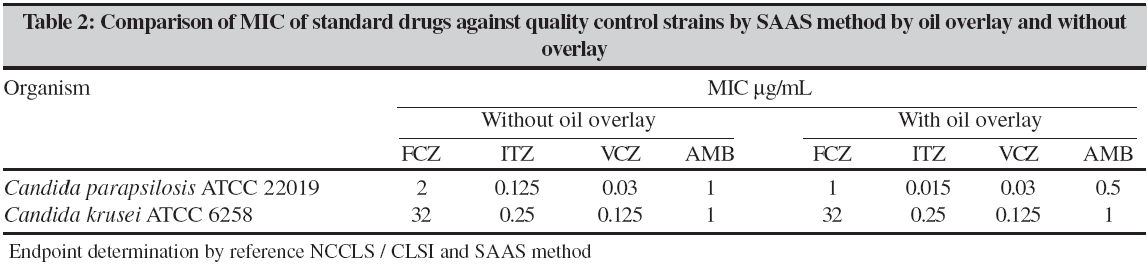
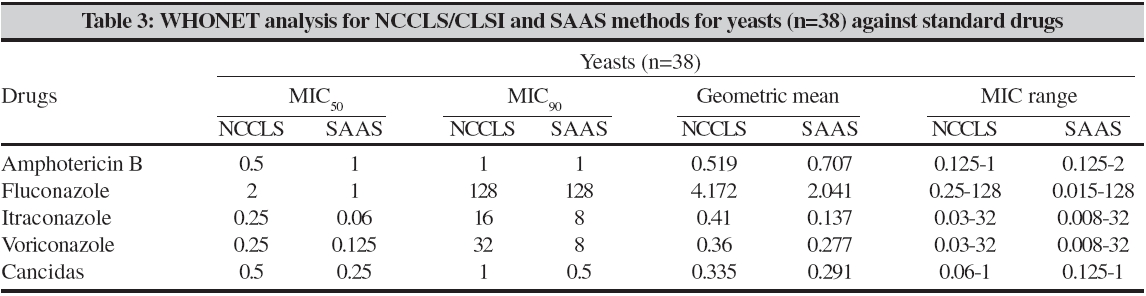
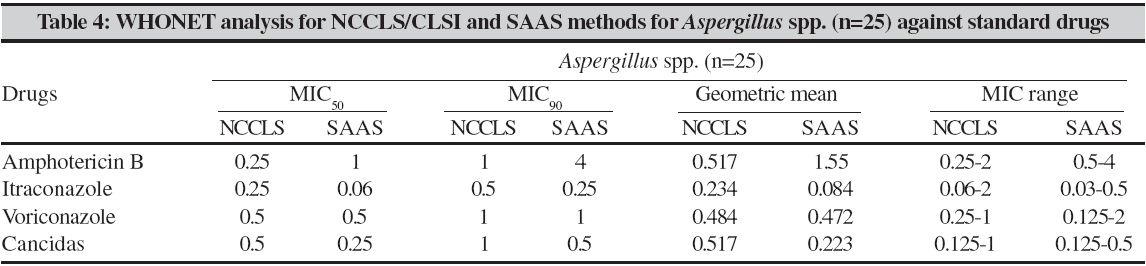
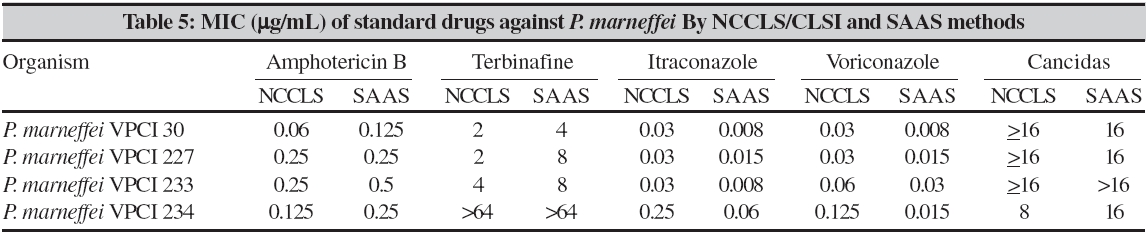
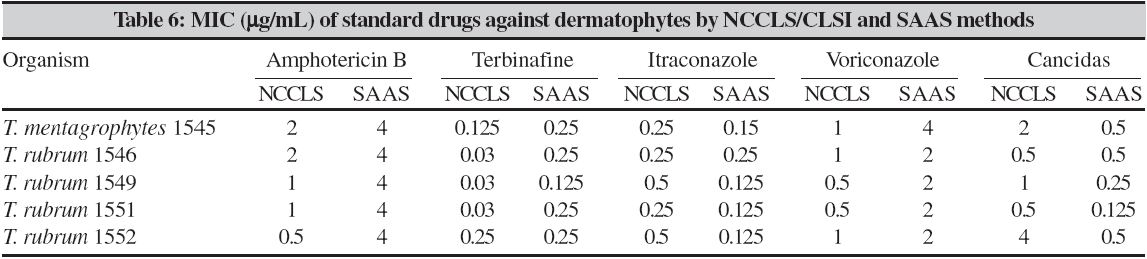
Inoculum preparation for SAAS Inoculation of drug containing tubes Endpoint determination Results Selection of medium for SAAS method In all three media MICs of FCZ and VCZ, against Candida parapsilosis ATCCC 22019 was in the NCCLS / CLSI recommended range. MICs of ITZ and AMB were either with in the range or one dilution higher, in case of RPMIA and BHIA. However, in SDA it was two dilutions higher. Candida krusei ATCC 6258 was also tested and it was observed that FCZ endpoint was above the NCCLS / CLSI range in SDA. All the media studied supported good growth but in SDA dense growth was observed which interfered with the end point interpretation. Though RPMIA and BHIA are comparable, BHIA was selected because of its low cost, availability and easy preparation. Effect of oil overlay on end-point determination by SAAS method MICs of 72 fungal isolates were determined by both NCCLS / CLSI and SAAS (BHIA without oil overlay). Comparison of NCCLS / CLSI and SAAS revealed that the MICs did not differ by more than one dilution for all drugs by SAAS. MIC 50 of NCCLS / CLSI and SAAS were in concordance (within 1 dilution) for the tested antifungal agents against all yeast and Aspergillus isolates [Table - 3][Table - 4]. However, MICs for yeast and Aspergillus isolates measured by the SAAS method predicted high susceptibility (reduced MIC) to both ITZ and CAN compared with the reference NCCLS / CLSI MIC [Table - 3][Table - 4]. The study was also extended to include P. marneffei and dermatophytes for MIC determination by both methods [Table - 5][Table - 6]. MICs against P. marneffei and dermatophytes suggests that SAAS is comparable to NCCLS / CLSI for susceptibility testing. However, in one P. marneffei isolate MIC of ITZ differed by almost three dilutions. Discussion Scientists from many laboratories have expressed their inability to determine antifungal susceptibility testing using the NCCLS / CLSI methodology. This leads to dependence of such laboratories on reference laboratories for antifungal susceptibility results leading to delay and /or inappropriate treatment. We have attempted to develop a simple method for determination of MIC of yeasts and molds for use in resource-constrained clinical microbiology laboratories and have compared its performance to the NCCLS / CLSI methodology. In NCCLS / CLSI M38-A spectrophotometric adjustment of conidial suspensions is recommended. To reduce the time required for antifungal susceptibility testing of filamentous fungi, SAAS method uses inoculum suspensions that can be readily prepared from the original pure plate. The test can even be set up as soon as the mold is isolated because only mycelial growth, the invasive form, can also be used as the inoculum unlike NCCLS / CLSI method, in which a calibrated conidial suspension only is recommended.[2] No special expertise or expensive equipment is needed, because the procedure is simple and similar for all fungi. Secondly, RPMI is recommended by NCCLS / CLSI for antifungal susceptibility testing however it is a synthetic, expensive, not routinely used medium in clinical microbiology (except tissue culture) laboratories and needs to be filter sterilized. SDB and BHI are comparatively cheaper, generally available in all clinical microbiology laboratories and no special expertise or equipment is needed for preparation. These three media supplemented with 0.5% agar were selected for evaluation of media for MIC determination of quality control strains by SAAS, as they are well-established fungal growth media. Reproducible susceptibility data against the two quality control strains were obtained in RPMIA and BHIA but BHIA was finally chosen because of its low cost, ease of availability and easy preparation in any microbiology laboratory. In the initial work on SAAS the investigators have used oil overlay on the inoculated tubes.[10],[11] This was done in order to mimic the growth conditions within the body, to control sporulation in filamentous fungi and to prevent contamination of medium in the tube (personal communication). However we found that the MICs were comparable in the presence and absence of oil overlay. During this study it was also observed that oil overlaying resulted in reduced growth even in the drug free tube. We considered the total growth and not just the growth inside the medium. Consequently, BHIA without oil overlay was selected for SAAS study. In order to assess the acceptability and accuracy of the SAAS, we determined MICs for 72 fungal isolates and compared the same by the new method with reference NCCLS / CLSI method. In addition, the SAAS MICs of quality control and reference strains were ≥95% in agreement with the recommended NCCLS / CLSI range. For ITZ, one or two isolates were out of the recommended range (1 dilution). In filamentous fungi, the MICs of reference strains ( A. flavus ATCC 204304 and A. fumigatus ATCC 204305) for AMB were in the NCCLS / CLSI ranges but were on the higher side of the recommended range. FCZ sensitive, intermediate and resistant yeasts chosen for the rapid-screening application of the SAAS method yielded consistent results. They correlated with the NCCLS / CLSI interpretive breakpoints of susceptibility. Susceptibility data of the tested clinical isolates (n=61, yeast and molds) to varying concentrations of antifungal agents is in agreement with the reference MICs. The application of the SAAS method, for the first time was also extended to antifungal susceptibility testing of clinical isolates of P. marneffei, a endemic pathogenic fungus of Southeast Asia specifically infecting patients with AIDS.[12] MICs obtained for the four P. marneffei clinical isolates by NCCLS / CLSI and SAAS did not differ by ≤two dilution for all the drugs. In P. marneffei VPCI 234, MIC of VCZ differed by three dilutions Dermatophytes were also used in this study and MICs obtained correlated well with the reference MIC (differ ≤two dilution). MIC for AMB and CAN for one isolate, T. rubrum 1552, showed a variance of 3 dilutions as compared to the NCCLS / CLSI MIC. For TER the NCCLS / CLSI and SAAS MICs differed by 3 dilutions in three strains. Statistical analysis of SAAS method showed 100% correlation with NCCLS / CLSI with respect to sensitivity, susceptibility positive and negative predictive value. SAAS method shows potential as a screen for antifungal susceptibility testing of yeasts and filamentous fungi. It is a simple method with no special expertise or expensive equipment. It is accurate and highly reproducible in our hands. It is inexpensive, may be performed on a single isolate and can be completed before final identification of the organism. A major advantage of the new method is its potential for screening both pathogenic yeasts and molds by same protocol. It appears from the data obtained by SAAS for antifungal susceptibility testing in this study that resource constrained clinical microbiology laboratories can benefit from this simple screening test. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06053t4.jpg] [mb06053t5.jpg] [mb06053f2.jpg] [mb06053t2.jpg] [mb06053t3.jpg] [mb06053t1.jpg] [mb06053t6.jpg] [mb06053f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}