 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 177-181 Original Article Molecular epidemiology of clinical isolates of AmpC producing Klebsiella pneumoniae Manchanda V, Singh NP, Shamweel A, Eideh HK, Thukral SS Department of Microbiology, University College of Medical Sciences, New Delhi - 110095 Code Number: mb06054 Abstract Purpose: AmpC producing K. pneumoniae have been increasingly reported from India but epidemiological studies are lacking. In the present study, molecular epidemiology of extended-spectrum AmpC beta-lactamases (ESACs) producing clinical isolates of K. pneumoniae prevalent in our hospital was studied.Methods: Fifty-one non-repeat, consecutive, clinical isolates of K. pneumoniae producing AmpC enzymes, were subjected to whole cell protein profile analysis (SDS-PAGE) and ribotyping. The antimicrobial susceptibility was determined using standard disk diffusion technique. The isolates showing decreased susceptibility to cefoxitin (<18 mm) or cefotetan (<16 mm) were subjected to modified three- dimensional test for detection of AmpC enzyme. Results: Six different types of protein profiles were observed. Ribotyping could further discriminate between the strains that were clustered by protein fingerprinting. Twelve different ribo-patterns were identified. Ribotyping was found to have a better Discriminatory Index (0.98) than that of SDS-PAGE (0.78). Of the 26 isolates that showed decreased susceptibility to cefoxitin and/or cefotetan 13 isolates were found to harbour AmpC enzyme. Conclusions: The study demonstrated the usefulness of SDS-PAGE whole cell protein profile analysis and ribotyping to identify the clonality of the ESACs isolates, the latter having a higher discriminatory power. The presence of ESACs isolates in the community as well as in hospital settings emphasizes the need for regular monitoring of antimicrobial resistance. Keywords: ESBL, ribotyping, SDS PAGE, protein fingerprinting, Klebsiella pneumoniae, AmpC Clinical bacterial isolates producing AmpC enzymes are resistant to oxyimino group (ceftazidime, cefotaxime, ceftriaxone and cefuroxime) and the 7a - methoxy group (cefoxitin, cefotetan, cefmetazole and moxalactam) cephalosporins. Several epidemiological studies have shown that AmpC enzyme producing bacteria are recovered from hospitalized patients after several days of admission to the hospital.[1]-[3] Affected patients have often had prolonged stays in intensive care units. These patients had surgical problems and one or more underlying chronic diseases. Source of organisms included urine (about 50% of the isolates), blood, wound, sputum or stool. A majority of patients had been treated with beta-lactam antibiotics including cefoxitin, moxalactam, cefotetan or imipenem.[1],[4] AmpC beta-lactamases are encountered most frequently in isolates of Klebsiella pneumoniae .[5] It is important to detect ESBLs producing as well as AmpC producing bacterial isolates since, there is a risk of the emergence of extended-spectrum AmpC beta-lactamases (ESACs).[6] Therefore, proper surveillance and epidemiological studies of such bacteria is of immense importance. AmpC producing K. pneumoniae have been increasingly reported from India but epidemiological studies are lacking.[7],[8],[9],[10],[11] In the present study, molecular epidemiology of AmpC producing clinical isolates of K. pneumoniae prevalent in our hospital was studied using sodium dodecyl sulphate polyacrylamide gel electrophoresis (SDS-PAGE) whole-cell protein profile analysis and ribotyping. Materials and Methods Bacterial strains Antimicrobial susceptibility testing Detection of AmpC enzymes Isolates found to harbour AmpC enzymes, were subjected to strain typing by whole cell protein profile analysis and ribotyping. SDS-PAGE whole-cell protein profiling Ribotyping Computerized numerical analysis of protein and ribo- patterns was performed using the diversity Database ® software (version 1.1) incorporated into a gel documentation system (pdi, USA). Cluster analysis of the patterns was done using the unweighted - pair group method with arithmetic averages - UPGMA. Even one band difference in protein profiles or ribo-patterns was taken as significant difference and the isolates were treated as different clones. The discriminatory power of the two techniques was calculated using numerical index called Index of Discrimination (ID), which is based on the probability that two unrelated strains sampled from the test population will be placed into different typing groups.[18] This probability was calculated by the following equation:
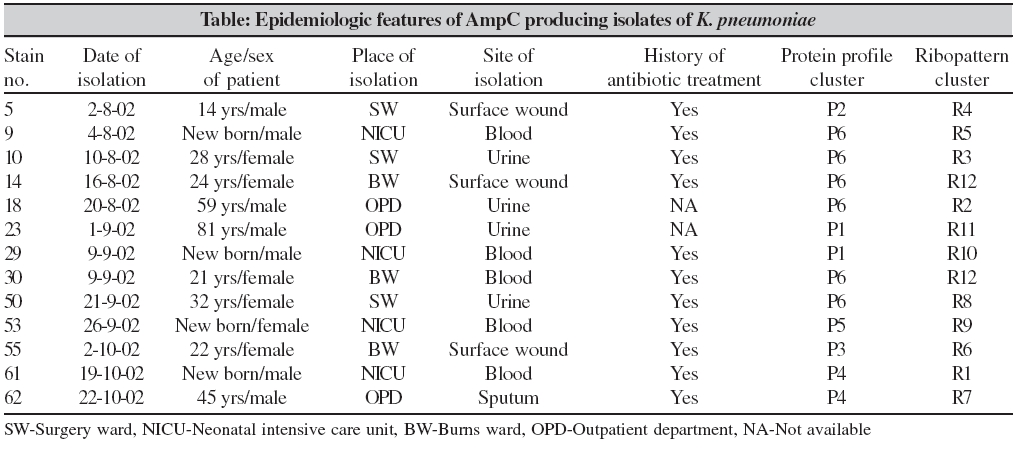
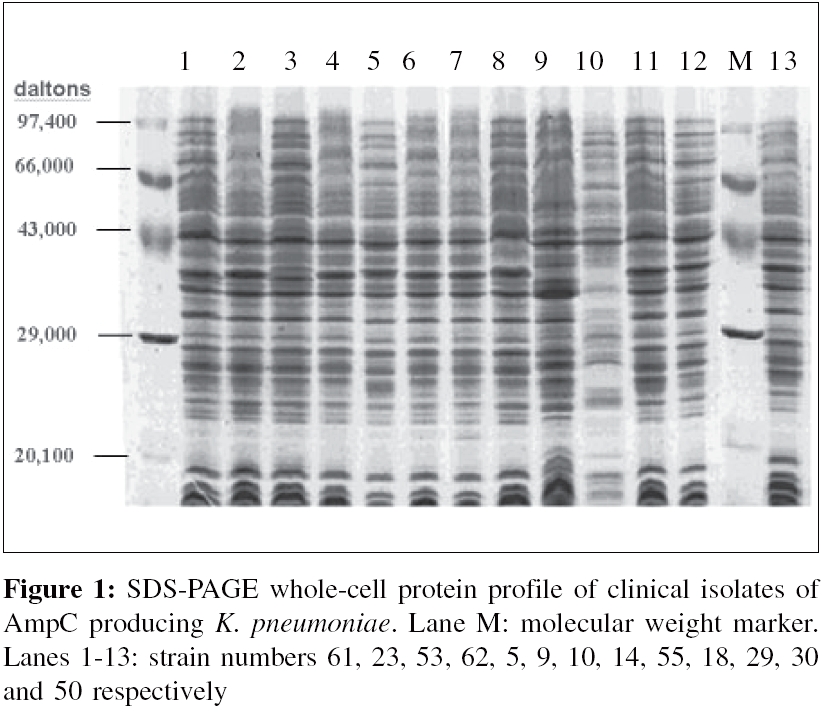
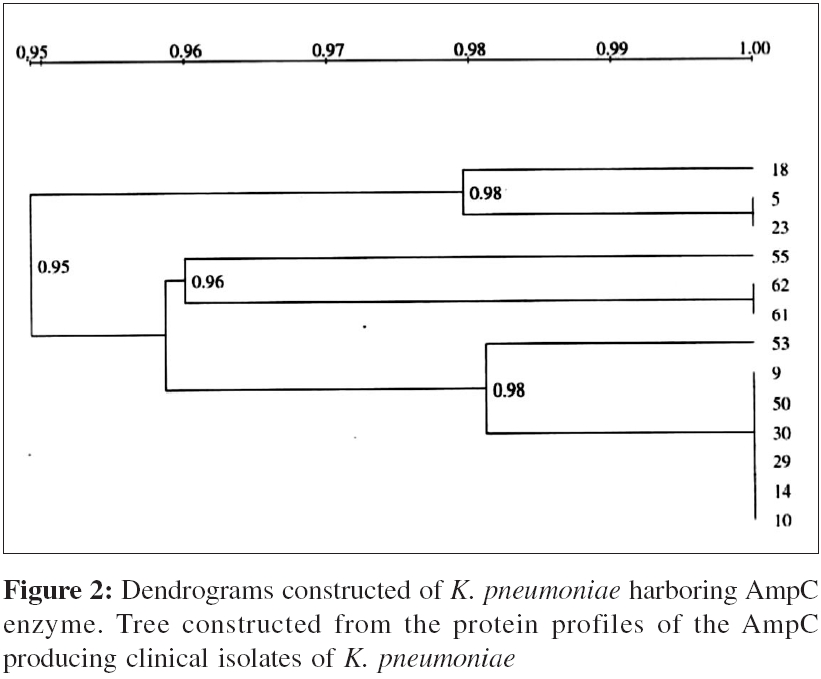
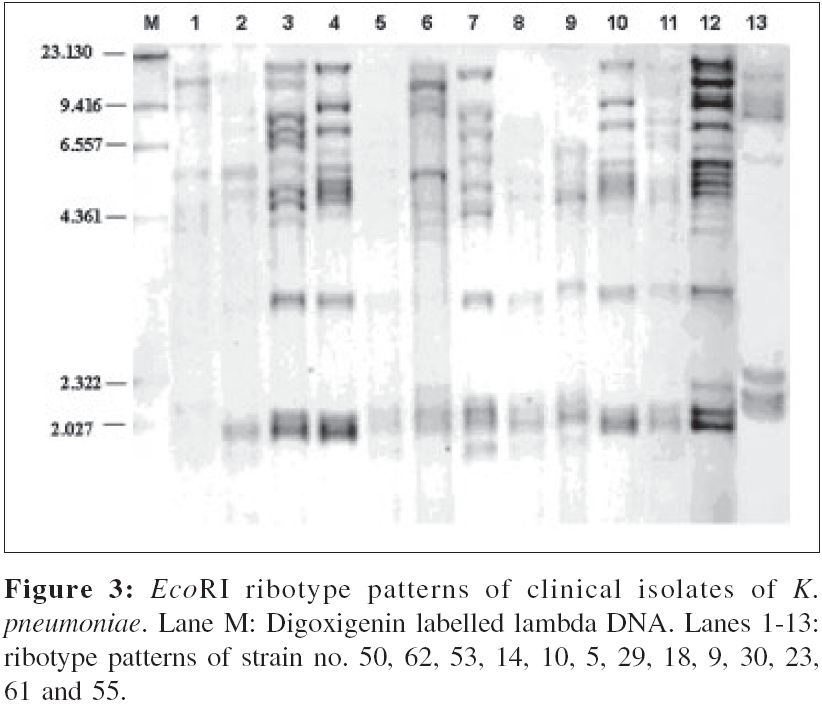
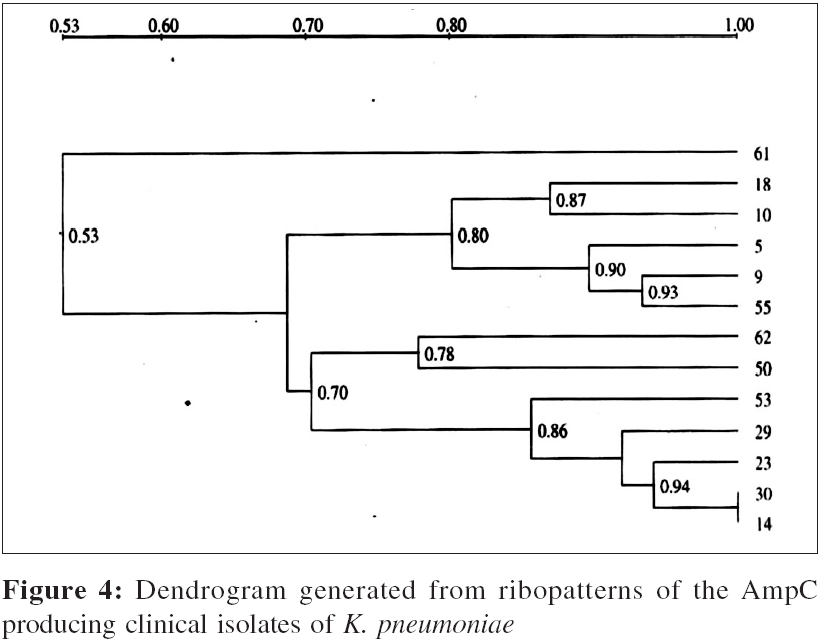
Where N is the total number of strains, s is the total number of types and nj is the number of strains belonging to the jth type. Results Epidemiological details of isolates are summarized in the Table. Whole cell protein profiles of these isolates had 32 to 38 protein bands [Figure - 1]. The dendrogram based on the similarity values of the protein profiles is shown in [Figure - 2]. Protein fingerprinting revealed six different types of protein profiles (P1 - P6). Protein type P6 was the largest cluster with six isolates. Ribo-patterns and the dendrogram based on similarity values of these patterns are shown in [Figure - 3] and [Figure - 4] respectively. The E co RI enzyme generated well-separated band patterns, which were easy to interpret because of moderate number of restricted DNA fragments (8 to 15) and their even distribution. The molecular weights of the fragments ranged between 20 to 0.5 kbp. Ribotyping could further discriminate between the strains that were clustered by protein fingerprinting. Twelve different types of ribo-patterns were identified. The technique showed that all AmpC producing isolates of K. pneumoniae were distinct clones except in one instance (ribo-pattern R12). Ribotyping was found to have a higher DI (0.98) than that of SDS-PAGE (0.78). Multidrug resistance (three or more drugs) was observed in 90% (n=46) of the isolates. Resistance to aminoglycosides was high, with as many as 72% (n=37) of the isolates showing resistance to gentamicin and 69% (n=35) to amikacin. Decreased susceptibilities to cefotetan and cefoxitin were observed among 51% (n=26) and 43% (n=22) of the isolates respectively. Of the 26 isolates that showed decreased susceptibility to cefoxitin and/or cefotetan 13 isolates were found to harbour AmpC enzyme. Discussion The present study demonstrates that most of the patients at our hospital were infected with distinct clones of ESACs. Origin of these ESACs could not be identified in our study. Presence of multiple clones of ESACs indicates that there was no patient-to-patient hospital transmission. Major risk factors for colonization or infection with ESACs have been shown to be long term antibiotic exposure, prolonged hospital stay, severe illness, residence in an institution with high rates of ceftazidime and other third generation cephalosporins usage and instrumentation or catheterization.[18],[19],[20] It has been shown in several studies that alimentary canal of patients gets colonized with such strains which then spread to the site of infection through the oro-faecal route.[21] Our study thus, points to the fact that several clones of AmpC harbouring K. pneumoniae were circulating in our hospital and these were involved in causing infection in different patients. Isolation of three AmpC positive clones from three patients of OPD is indicative of the extent of circulation of such strains in the community. All the hospitalized patients from whom isolates producing AmpC enzymes were isolated had a history of intake of antibiotics. Unfortunately, history of antibiotic intake of OPD isolates was not available. This data emphasized the need of stricter implementation of antibiotic policy in the hospital and the need of continuous surveillance of antimicrobial resistance among the hospital and community isolates to curb the emergence and spread of ESACs. SDS-PAGE whole-cell protein profile analysis was used for the first time by Costas et al , for typing clinical isolates of Klebsiella aerogenes.[14] The protein patterns were reported to be highly reproducible and were used as the basis of numerical analysis, which divided the clinical isolates into various protein types. It was concluded that high-resolution SDS-PAGE of proteins provides an effective adjunct to other methods for typing isolates of K. aerogenes . SDS-PAGE whole cell protein profiling has never been used earlier for typing of AmpC producing K. pneumoniae isolates. Our study is the first study of its kind in which this technique has been evaluated. The technique was able to discriminate between the unrelated strains with DI of 0.78. Only a few studies on ribotyping of K. pneumoniae for delineation of the epidemiology are available in the literature. In a study, 14 clinical isolates of K. pneumoniae , isolated from different hospitals of France between 1987 and 1989, were subjected to different typing techniques including ribotyping.[22] Ribotyping with Eco RI and Hin dIII and genomic fingerprinting with Xba 1 by PFGE were concordant and suggested that 12 of the isolates recovered from the 14 hospitals were probably the same strain. In the present study, ribotyping could identify two strains belonging to the same clone (R12). Protein fingerprinting also clustered these two isolates in one protein type (P6). Both of these isolates were obtained from the burns ward with a gap of almost three weeks. The source of infection could not be identified. It can be concluded that majority of patients in our hospital were infected with different clones and there was no evidence of patient to patient transmission during the period of this study. The study also demonstrated the usefulness of SDS-PAGE and ribotyping as epidemiologic typing techniques; the latter being more discriminatory. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06054t1.jpg] [mb06054f3.jpg] [mb06054f2.jpg] [mb06054f4.jpg] [mb06054f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}