 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
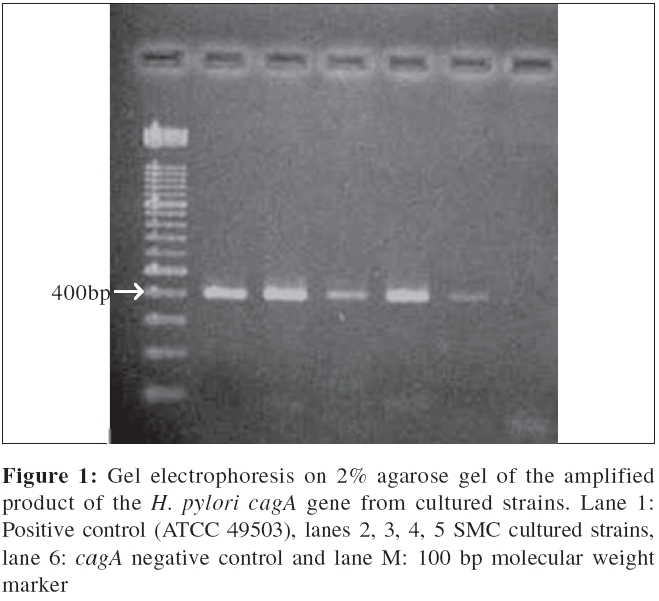
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 195-200 Original Article Detection of Helicobacter pylori cagA gene in gastric biopsies, clinical isolates and faeces Bindayna KM, Al Baker WA, Botta GA Department of Microbiology, Immunology and Infectious Diseases, College of Medicine and Medical Sciences, Arabian Gulf University, Kingdom of Bahrain Code Number: mb06057 Abstract Purpose: Helicobacter pylori infection is common in the developing countries. The cagA gene is a marker of pathogenicity island (PAI) in H. pylori . The aim of this study was to determine the prevalence of cagA among dyspeptic patients in Bahrain directly from gastric biopsy and stool specimen.Methods: A total of 100 gastric biopsy samples, 16 clinical isolates and 44 faecal specimens were collected from Bahraini adult dyspeptic patients. cagA gene of H. pylori was assessed using polymerase chain reaction (PCR). Results: The cagA gene was detected in 59 (59%) from biopsy specimens, 10 (62%) clinical isolates and in 10 (22.7%) faecal specimens. The detection of cagA positive H. pylori was significantly higher in patients with duodenal ulcer (80%) compared to those with other endoscopic finding (42%) ( P <0.05). Conclusions: Using PCR to detect cagA gene directly from biopsy is a rapid and reliable technique. However, using stool specimen for genotyping in our patients showed reduced sensitivity. Keywords: CagA gene, gastric biopsy, Helicobacter pylori, stool Helicobacter pylori is a gram negative spiral bacterium that colonizes the human stomach. Infection with H. pylori is associated with chronic gastritis, peptic ulcer, gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue lymphoma.[1] Two major bacterial virulence markers of H. pylori , the vacuolating toxin (VacA) and the cytotoxin-associated gene product ( cagA ), may play a major role in determining the clinical outcome of Helicobacter infections.[2],[3],[4] The VacA gene, which is present in all H. pylori strains, contains at least two variable regions, the signal(s) region and middle region(s). The subtype s1/m1 strains produce a higher level of cytotoxin activity than other genotypes.[4] The cagA , which is not present in every H. pylori strain,[5] is a marker for a pathogenicity island[6] and associated with more severe clinical outcomes.[2] A strong association between cagA and vacA signal sequence type s1 has been reported.[4] Polymerase chain reaction (PCR) has been successfully used to detect H. pylori cagA and vacA virulence genes in gastric biopsies. The potential advantages of PCR include high specificity, quick results and the ability to type bacteria without the requirement for special transport conditions. Studies show that a novel PCR method was successfully performed to detect H. pylori DNA using specific genes such as 16SrRNA,[7] vacA s1 and cagA directly from gastric biopsies to detect pathogenic H. pylori.[8] It is also has been proven to be useful in the detection of H. pylori in other biological products, such as gastric juice, saliva, dental plaque and faeces.[9],[10] Although this test has high sensitivity and specificity,[11] practical consideration and cost have limited its use.[12] Stool PCR analysis appears to be a rapid and accurate noninvasive tool for detecting H. pylori , especially in children. H. pylori DNA has been detected in faeces of infected humans by using PCR to amplify genes such as the ureA and ureC genes[13] and the 16S rRNA gene.[14] However, the results obtained using stool DNA as templates for PCR are variable and depend on factors such as the amount of recovered intact DNA, the techniques used for microbe concentration as a pre-PCR step, techniques used for removal of faecal inhibitors, as well as the amplification protocols used. The present study represents the first in Bahrain to detect H. pylori cagA from gastric biopsy, clinical isolates and stool samples using PCR-based methods. Materials and Methods Study subjects Between April and September 2001, a total of 100 consecutive informed and consenting adult patients with dyspeptic symptoms were recruited for the study. These patients were referred by their physician for diagnostic upper gastrointestinal endoscopy in Salmaniya Medical Complex (SMC), Manama, Kingdom of Bahrain. The patients had not received nonsteroidal antiinflammatory drugs, antacids or antibiotics in the two months prior to examination. None of the patients underwent colonoscopy at least one week prior to collection of stool specimens. Gastric biopsies were collected from all subjects. Stool specimens were collected from 44 patients in a sterile container and were transported the same day to the laboratory in dry ice and kept at -80°C until the DNA extraction and PCR were preformed. Patients′history and endoscopy findings were obtained from case files. Endoscopy All patients underwent endoscopy and biopsies were collected by the gastroenterologists, who independently described the endoscopic appearance of the stomach and the duodenum. A Pentax (C122336, Japan) or an Olympus endoscope (2715038, USA) was used. Two biopsies were taken from each patient, one from the gastric antrum and the other from the corpus and transported immediately to the laboratory in normal saline for molecular analysis or kept frozen in 15% tryptone soy broth (Oxoid Ltd., Basingstoke, England) and stored at -80°C until analysed. Between endoscopies, endoscopes and biopsy forceps were disinfected using standard methods. The endoscopic findings were described as normal, gastritis, chronic gastritis, gastroesophageal reflux (GER), duodenitis and duodenal ulcer. Bacterial strains Sixteen H. pylori strains were obtained from the Microbiology laboratory of Salmaniya Medical Center (SMC), Bahrain. These strains had been cultured at 37°C on 5% sterile sheep blood (Oxoid Ltd. Basingstoke, England) and incubated at 37°C for up to 3-5 days in a microaerobic condition using a gas generator kit (Gas Camp Campylobacter system, Oxoid Ltd., Basingstoke, England). H. pylori identification was based on morphology, Gram stain, Oxidase, catalase and urease tests. All the isolated H. pylori were kept frozen at -80°C in the tryptone soy broth medium containing 15% (vol/vol) glycerol until DNA extraction was performed. These clinical isolates were used as controls for comparison with H. pylori DNA extracted from biopsy and faecal specimens. The reference strain (ATCC 49503) kindly provided by Dr. J. Rudi (Medizinische Klinik und Poliklinik, Heidelberg, Germany), was used throughout the study as a positive cagA control. DNA isolation Culture of H. pylori was harvested in phosphate buffered saline for DNA extraction. The pelleted cells were resuspended in 200 mL of proteinase K solution (10 mM) Tris-Hcl (pH 7.8), 5 mM EDTA, 0.5% sodium dodecylsulfate (SDS), 50 mg of proteinase K per mL) and the mixture was incubated at 55°C for 30 minutes. The DNA was extracted with phenol-chloroform-isoamyl-alcohol by standard procedures. Gastric biopsy specimens were homogenized in 200 mL of proteinase K with a sterile micro-pestle (Eppendorf, Hamburg, Germany). DNA was isolated from the homogenate by use of QAamp DNA kit (QIAGEN, Hilden, Germany) according to the manufacturer′s instruction and DNA stored at -20°C until analysis. Rapid DNA isolation from both fresh and frozen faecal specimens was performed with the QIAamp DNA stool mini-kit (QIAGEN) according to the manufacturer′s instruction. The final eluate was stored at -20oC until analysis. The amount of total DNA isolated from biopsy, clinical isolate and stool samples were 28-143.5 ng/mL, 60-200 ng/mL and 55.2-190.5 ng/mL respectively. Polymerase chain reaction Extracted DNA samples were amplified using Gene Amp Amplicore ® PCR core reagents kit (Perkin Elmer, N808-0009, Roche. USA), PCR was carried out in 50 µL volumes containing: 10 mM Tris-Hcl (pH=8.3), 50 mM Kcl, 1.5 mM MgCl 2, 200 mM of each dNTPs, 50 pmol of each primer, 2.5 units Taq polymerase and 5 µL DNA template extracted from strains and biopsy or 1.5 µL extracted from faeces. Specific primers (5′-AATACACCAACGCCTCCAAG-3′) and (5′-TTGTTGCCGCTTGCTCTC-3′) (Interactiva, England) were used to amplify a 400bp fragment from the cagA gene (20481-20880). The amplification reaction was carried out in GeneAmp PCR system 9700 (applied biosystem; Perkin Elmer; Norwalk, USA) with a program consisting of an initial denaturation step at 94°C for 4 minutes and 35 cycles of denaturation at 94°C for 1minute, annealing at 59°C for 1minute and an extension step for 1minute at 72°C and a final extension step at 72°C for 10minute. A 10 mL of PCR products was then analyzed by electrophoresis on 2% agarose gels run in acetate EDTA (TAC) buffer and stained with ethidium bromide. The PCR product was examined in parallel with molecular size marker 100-bp DNA ladder (Boehringer Mannheim, Germany). Analytical sensitivity of stool PCR In order to evaluate the sensitivity of the detection of cagA gene from faecal samples, a stool sample previously demonstrated to be H. pylori free was artificially inoculated with the cagA positive control strain (ATCC49503) obtained from 3 day-old culture in nonselective medium. In particular, a suspension of above mentioned strain equivalent to 0.5 opacity on McFarland scale (corresponding to 1.5 x 10 6 CFU/mL) was prepared in sterile H 2 O and 10 μL of this suspension, 10 μL of a 10 fold dilution (15000 CFU) of this suspension (1500 CFU) and, 10 μL of 100 fold dilution of the suspension (150 CFU) and final 10 μL of 1000 fold dilution of the suspension (115 CFU) were added to faecal samples (each 220 mg). Following the additions, the samples were homogenized and analyzed following the PCR protocol described above. Data analysis Fisher exact test was used for analysis of data. A P value of < 0.05 was accepted as statistically significant. Results Subjects The mean age of the patients was 44 years (standard deviation, 15.5 years; range, 16-77 years). Of the 100 patients, 44 (44%) were male and 53 (53%) were female. Bacterial clinical isolates A total of 16 H. pylori isolates were tested by PCR assay after phenol-chloroform extraction. Ten isolates were marked positive by amplifying the expected 400bp fragment, which detects the cagA gene; therefore, they were considered as cagA positive producing H. pylori strains [Figure - 1]. Analytical sensitivity of stool PCR The sensitivity of PCR method was evaluated by testing the faecal sample (previously demonstrated to be H. pylori free) artificially inoculated with a suspension of cultured cagA positive H. pyloro strain containing 15,000 CFU, 1500 CFU, 150 CFU or 15 CFU. The detection limit of the PCR method was 1500 CFU; no PCR product was obtained from fecal sample inoculated with 15 CFU of H. pylori [Figure - 2]. Endoscopy finding and cagA association Endoscopic examination was performed on all 100 patients. Abnormal findings were observed in 81 (81%) of the patients. Gastritis was found in 46 (46%), duodenitis in 15 (15%), duodenal ulcer and gastroesophageal reflux (GER) in 10% of patients. As shown in the table, association between cagA status and the endoscopic features of patients significantly correlated with duodenal ulcer GER patients (80%) ( P < 0.05). PCR for biopsy The expected 400bp amplication was found in 59 (59%) biopsy samples, which were considered as positive, while it was absent or showed nonspecific bands in 41 (41%) samples, which were considered negative for the cagA gene [Figure - 3]. Among nineteen patients with normal endoscopy findings, eight patients were found to be cagA PCR positive when biopsies were examined. Additionally, eight biopsies were found to be cagA PCR positive among 10 patients diagnosed with gastroesophageal reflux (GER), which is considered to be a high percentage rate (80%). The Table shows the level of cagA positivity detected in patients with different endoscopic findings. Among the 40 patients suffering from gastritis, 19 (47%) had a PCR cagA positive biopsy. Sixty-seven percent of duodenitis patients showed positive biopsy PCR. PCR for faeces The cagA gene was only detected in 10 out of 44 (22.7%) stool samples while 34 (77.2%) of these samples were negative. Discussion Bacterial DNA can be used as a marker for infections. Under ideal circumstances, the sensitivity is close to that of culture. The potential advantages of PCR include high specificity, quick results and the ability to type bacteria, whether they were in a viable form or not, but practical considerations and cost have limited its use.[12] Detection of H. pylori by PCR from non-biopsy samples has been done recently in research laboratories and in private laboratories because it is a non-invasive method and because of its rapid nature, especially when results are needed for emergency cases. H. pylori DNA was isolated from gastric biopsy,[8] gastric juice,[15] saliva, dental plaque[16] and recently from faeces[17] using universal primers coding for genes that are common to all H. pylori strains. In light of the effectiveness of these techniques, we decided to extract H. pylori DNA from gastric biopsy specimens, clinical isolates and stool and amplify the positive cagA gene directly from these specimens using a universal single set of primers. The cagA gene which is encoded for by cag PAI has been described as a marker for pathogenic H. pylori strains and has genes homologous to those of the type IV secretory pathway. This pathway encodes a secretion system involved in the export of virulence determinants and influences the secretion of IL-8, involved in the severity of the disease. Furthermore, studies suggested that there is a correlation between the prevalence of cagA seropositivity and peptic ulcer disease and gastric cancer.[18] In this study cagA positive strains were found in 59 (59%) biopsy samples, 10 (62%) clinical isolates and in 10 (22.7%) were fecal samples. The prevalence of cagA positive H. pylori strains varies from one geographic regions to another, e.g, 72% in Germany, 67% in Netherlands, 48% in Sri Lanka, 81 in United States, 93% in Nigeria and 97% in Korea.[8] cagA positive H. pylori strains have been known to be associated with severity of disease outcome.[19] The results obtained from our study were consistent with results of the previous study, showing a significant correlation ( P < 0.05) between cagA isolated from biopsy and endoscopy findings [Table - 1]. The most significant results were that pathogenic H. pylori was detected in 80% of duodenal ulcer patients and 100% of chronic gastritis patients, a result that was perfectly consistent with results obtained from the Chinese population showing 95% positive cagA gene with peptic ulcer disease and 100% with chronic gastritis.[19] Our study shows the presence of the cagA H. pylori gene in 8 out of the 19 (42%) patients that were endoscopically diagnosed as normal. The most likely explanation is that the type IV secretion apparatus in the pathogenic H. pylori isolated from these patients might be switched off or defective.[20] Another explanation is that the immune system of these individuals might be defective or the general immunity is low for some reason; for example, patients suffering from HIV in urban African areas had reduced risk of gastroduodenal mucosal lesions because Th1 and CD4 cells were paralyzed by HIV virus or by other intestinal nematodes. It has been noted before that these immune system cells have an important role in gastric inflammation.[21] Studies found a negative association between the presence of positive cagA and oesophageal disease.[18] The role of H. pylori in gastroesophageal reflux (GERD) is still controversial and the role of virulence markers of the bacterium has not been evaluated in most studies of GERD. In our study the gene of cagA was found in 80% of GERD patients, compared to another study which also showed a high percentage (66.9%) of GERD patients with positive cagA gene. In the same study, positive cagA gene strains were associated with more intense gastritis.[22] When the infection was contracted is important, in our opinion, especially because H. pylori is known as a life-long infection and it colonizes the human stomach for a long period of time until it causes severe infections;[23] thus, individuals might been infected recently and more severe complications have yet to be produced. The other consideration will be where they acquired the infection. Evidence of geographical variations has been reported for the cagA gene and this is associated with the disease outcome. A study by Yamaoka and colleagues found that there is variability in the structural organization of the 3′region of cagA and it is associated with the severity of the disease.[24] It differs markedly among different populations while it is conserved within the same population.33 For example, the primary cagA region in Japan differs from the cagA region for Western isolates.[24] The association of cagPAI with disease status was about 90% in India, a value higher than in Western countries, where it has been found to be 60%[18] and it is lower than in East Asia.[25] Detection of H. pylori in faeces using PCR and standard extraction methods has proved difficult, producing erratic results due to a variety of faecal inhibitors, such as acidic polysaccharides, metabolic products and large amounts of irrelevant DNA, which compromise the sensitivity of PCR. For this reason, DNA extraction procedures that remove inhibitors of PCR and concentrate the pathogen or total DNA were developed, such as filtration of stool specimens by using polypropylene filters, use of extraction kits QIAamp for tissue and stool and recently use of immunomagnetic beads for separation of inhibitors.[26] The prevalence of positive cagA gene extracted from patients′ stool, in this study, was low showing only 10 (22.7%) out of 44, when compared to biopsy and clinical isolates. Other studies showed a higher prevalence of 60%, however they were using different DNA extraction method which may explain the lower sensitivity. In conclusion, PCR assay for detection of H. pylori cagA is more reliable in biopsies than from stool. This study shows the importance of differentiating between pathogenic and non-pathogenic strains using cagA gene typing by PCR. Analysis of the results indicates that environmental, geographical and immunological factors may influence the outcome of H. pylori infection. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06057t1.jpg] [mb06057f1.jpg] [mb06057f3.jpg] [mb06057f2.jpg] |
| |||||||||
{kind=link}
![[Figure - 2]](/showimage?mb/photo/mb06057f2.jpg){kind=link}
![[Figure - 3]](/showimage?mb/photo/mb06057f3.jpg){kind=link}
![[Table - 1]](/showimage?mb/photo/mb06057t1.jpg){kind=link}