 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
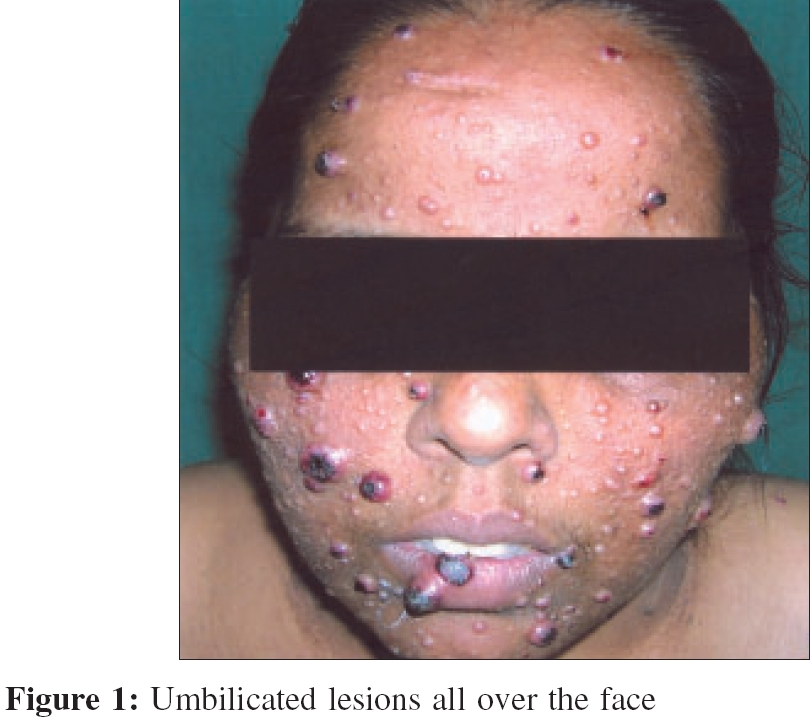
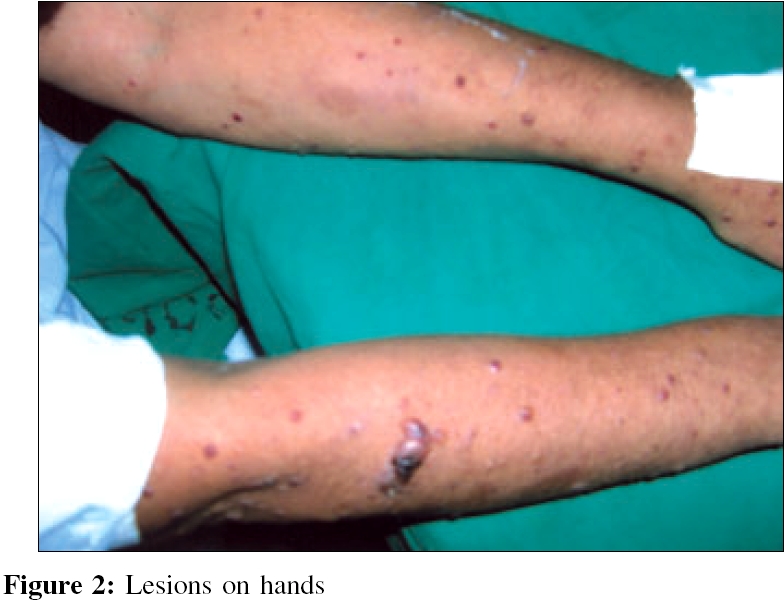
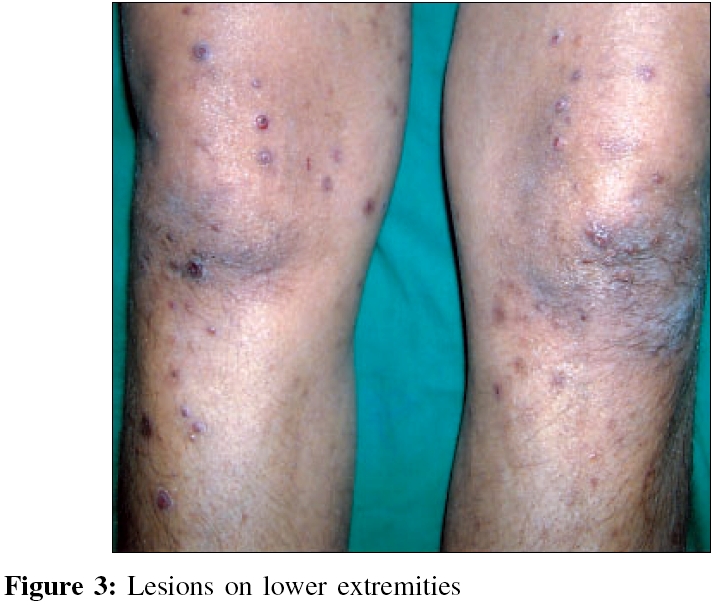
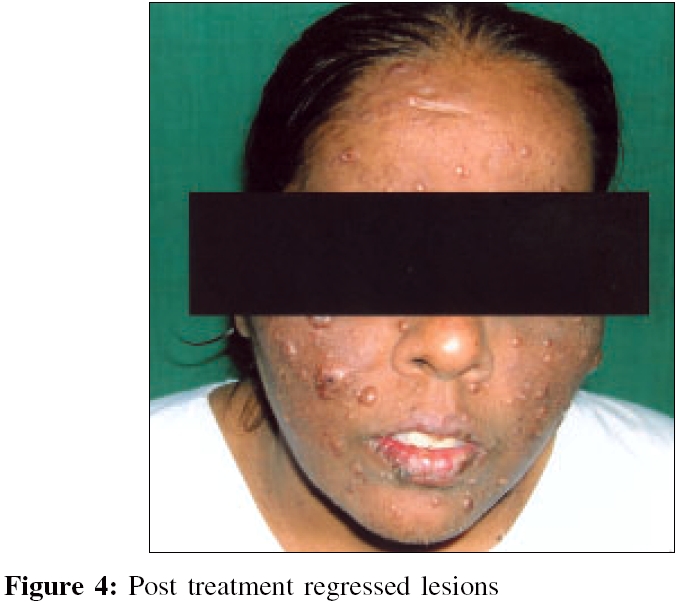
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 228-230 Case Report Disseminated crytococcosis with extensive cutaneous involvement in AIDS Dharmshale SN, Patil SA, Gohil A, Chowdhary A, Oberoi C Department of Microbiology, Grant Medical College and Sir J J Group of Hospital, Mumbai - 400 008 Code Number: mb06066 Abstract Cutaneous infections is observed in 15% of patients with disseminated cryptococcosis with AIDS. We present here a case of a 34 years old female with AIDS. She presented with multiple skin coloured umbilicated over face, neck, trunk and limbs, which mimicked molluscum contagiosum and kaposi sarcoma. The tissue from cutaneous lesions was collected by excision biopsy and processed by standard mycological methods. Cryptococcus neoformans was isolated and identified. Cerebrospinal fluid (CSF) also yielded the growth of C. neoformans . Cryptococcal antigen was detected with a titre of 1024 by Latex agglutination, is serum and CSF. Her serum was reactive for HIVI and 2 antibodies. The CD4 lymphocytes count was 80/cmm. The HIV viral load was 2,48,084 copies/mL. She was treated with amphotericin B injectable and oral fluconazole. She responded well and lesions regressed.Keywords: Acquired immunodeficiency syndrome, cutaneous cryptococcosis Cryptococcosis is a systemic infection caused by the encapsulated yeast, Cryptococcus is ubiquitously found in the soil, in pigeon droppings and in their nesting places. Its usual route of entry into humans is via inhalation of non-or poorly encapsulated form of the organism. Even though the lungs are the sites of inoculation, pulmonary infection in the immunocompromised tends to be asymptomatic.[1] It occurs in 6 to 13% of patients with acquired immunodeficiency syndrome (AIDS), when their CD4 lymphocyte count is below 200/cmm.[2] Before the AIDS epidemic, most cases of cryoptoccosis were related to cancers, especially lymph reticular malignancies. Treatment with corticosteroid agent and sarcodiosis has been linked to cryptococcal disease. There are reports of cryptococcosis in HIV negative patients with history of splenectomy and organs transplantation. Currently, AIDS represents the most common risk factor for the development of cryptococcosis. Cryptococcosis at other sites follows dissemination from the lungs, Cryptococcal meningitis that follows typical subacute course represents most frequent clinical manifestation. The cutaneous involvement and others like endophthalmitis, chorioretinitis, conjunctivitis, sinusitis, myocarditis, pericarditis, endocarditis, gastroduodenitis, hepatitis, cholecysitis, peritonitis, renal abscesses, adrenal involvement, arthritis, osteomyelitis, lympadenitis and breast masses etc. have also been reported.[2] The skin is most common extra-neural site of infection, affecting 10-20% of those with systemic involvement.[3] The lesions vary greatly in morphology and mimic other dermatological entities.[3] They may be misdiagnosed as molluscum contagiosum and Kaposis sarcoma.[1],[2],[3],[4] The lesion may appear as papules, tumors, vesicles, plaques, abscess, cellulitis, purpura, draining sinus, ulcers bullae or subcutaneous swelling.[1],[3],[4] These lesions are an ominous sign as they are often the first presenting symptom of systemic disease. However, rare case of primary inoculated cutaneous lesions, without evidence of disseminated disease, has been reported.[3] Case Report A 35-year-old female patient came with multiple raised asymptomatic lesions over face, neck, extremities and back since 20 days (Figs. 1,2and3). She gave history of severe headache with vomiting and fever since ten days. No past history of diabetes, hypertension, herpes zoster and jaundice was present. She had a history of pulmonary tuberculosis one year back for which she had taken anti-tuberculous treatment for six months. She, her husband and their thirteen-year old child had been detected as HIV seropositive. Therefore, she was provisionally diagnosed as disseminated cryptococcosis histoplasmosis/penicillosis/molluscum contagiosum with AIDS. Initial cerebrospinal fluid (CSF) examination for cryptococci was found to be negative for microscopy and culture. Skin excision biopsy and cutaneous issue revealed plenty of budding yeast cells with demarcated capsules of 5-10 mm size by India ink preparation (IIP) (Fig. 4) and Gram staining. Specimens were inoculated on Sabouraud dextrose agar (SDA) and incubated at 37° C and room temperature (RT). On SDA, creamy flat, shiny, moist mucoid colonies were grown with smooth edges. Luxuriant growth on SDA at RT was observed in 2 days. The CSF received after 10 days was found to be positive for budding yeast cells by microscopy and Cryptococcu s was grown on SDA. Urine sample showed a single yeast cell observed by microscopy in IIP, but SDA did not yield growth. The blood culture and sputum specimens were negative by microscopy as well as culture. Cryptococcal isolates from different clinical specimens were further confirmed by IIP and crushed urease test. All the isolates were confirmed as Cryptococcus neoformans. Cryptococcal antigen was detected in CSF and serum by latex agglutination test in the titre of 1024. The immunophenotyping studies of her lymphocytes revealed, total lymphocyte count-5500, absolute lymphocyte count-654/cmm, absolute CD3-232/cmm (35.5%), CD4-80/cmm (12.3%) and CD8-185/cmm (28.3%). HIV viral load assay in patient′s serum was shown to have 2,48,084 copies of RNA/mL. She was treated with amphotericin B injection 0.7 mg/kg for 14 days, then shifted to fluconazole 200 mg twice daily for eight weeks. This was followed by maintenance dose of oral fluconazole (200 mg) once a day. She responded very well to the treatment and the lesions regressed completely.Discussion Cryptococcal infection in AIDS manifests with meningoencephalitis, pneumonia or disseminated disease. Cutaneous cryptopcoccosis is observed to be in 10-15% patients. The numerous umbilicated papules developing in HIV seropositive patients leads to differential diagnosis of molluscum contagiosum, penicillosis, histoplasmosis and cryptococcosis.[2],[4],[5] India ink preparation, Gram stain, growth on SDA of excision biopsy, cutaneous tissue and the titer of 1024 cryptococcal antigen in serum and CSF by latex agglutination test, confirmed the diagnosis. It is indicative of systemic disease and correlates with fungal burden. Our case report and the investigations correlate with those reported by other authors.[4],[5] Early diagnosis by microscopy, culture and then serology helps in starting immediate treatment for disseminated cryptococcosis. Fluconazole has been found to be particularly effective due to its high bioavaibility, excellent CSF penetration and long half-life. Therefore, it is regarded as the drug of choice for prophylactic therapy. The mortality of disseminated cryptococcosis is 70-80% in untreated patients compared with those treated with systemic antifungal agents.[3] References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06066f4.jpg] [mb06066f1.jpg] [mb06066f3.jpg] [mb06066f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}