 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
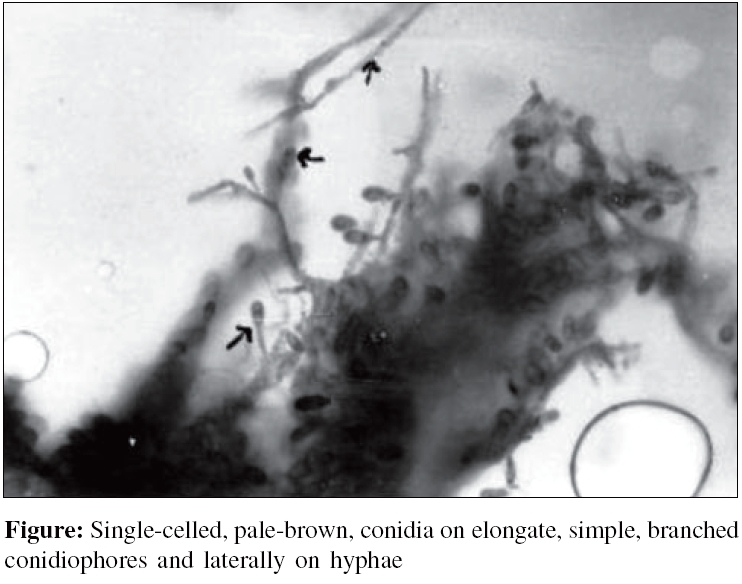
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 231-232 Case Report Brain abscess due to Scedosporium apiospermum in a non immunocompromised child Acharya A, Ghimire A, Khanal B, Bhattacharya S, Kumari N, Kanungo R Department of Clinical Microbiology, Pondicherry Institute of Medical Sciences, Pondicherry - 605 006 Code Number: mb06067 Abstract Scedosporium apiospermum is a filamentous fungi that commonly causes cutaneous infection. In certain circumstances, S. apiospermum can also cause invasive disease, which can involve the central nervous system (CNS). When the CNS becomes involved, treatment is difficult, therapeutic options are limited and the prognosis is poor. Early identification and treatment can decrease the mortality rate. Here we present a case of brain abscess with chronic suppurative otitis media, caused by S. apiospermum . This is the first such case report from Nepal. We could identify the organism only post mortem. We could not save the patient, probably due to delay in diagnosis.Keywords: Brain abscess, chronic suppurative otitis media, Scedosporium apiospermum Scedosporium apiospermum is a soil saprophyte of low virulence.[1] Majority of infections due to this fungus result in mycetoma. Other infections are localized to paranasal sinuses, lungs, ears and eyes. Scedosporium apiospermum do not usually invade tissues and vessels in the immunocompetent. Damage by this organism is only by severe local reaction. In the immunosuppressed individuals tissue and vascular invasion is commonly seen.[2] Brain abscess due to Scedosporium apiospermum has been reported from various parts of the world.[3] This is the first report from Nepal. Case Report A 12 year-old female child was admitted to the paediatric ward with complaints of fever, headache, earache and vomiting for four days. There was history of neck pain and drowsiness for two days. There was no history of trauma or convulsions. She gave a history of left ear discharge off and on since childhood. Physical examination revealed the patient to be conscious and well oriented. Chest, CVS, P/A examination was normal. Neck rigidity was present, Kerning′s signs were elicited. A provisional diagnosis of chronic suppurative otitis media (CSOM) with meningitis was made. Routine haematological and blood parameters were normal. Chest X-ray was normal. X-ray of mastoid showed radiolucent cavity in left mastoid. CT scan of the brain revealed multiple brain abscesses in left temporal lobe. Diagnosis of a chronic suppurative otitis media with complicated by brain abscess was made. A modified radical mastoidectomy was done and extradural abscess was drained. Perioperative finding was cholesteotoma with extradural abscess. Thick purulent discharge was drained and sent to microbiology laboratory for culture. The aspirated material was subjected to microscopic examination which showed plenty of inflammatory cells but no micro-organisms. No pyogenic organisms were isolated on routine bacteriological media. Fungal culture showed mousy gray colour velvety colony with short arial hyphae with a greyish-black reverse on Sabouraud′s dextrose agar after 72 hours of incubation. Lactophenol cotton-blue mount showed numerous single-celled, pale-brown, conidia borne singly and in small groups on elongate, simple and branched conidiophores or laterally on hyphae (Fig.) Routine cytology and biochemistry did not show any abnormality in the cerebrospinal fluid (CSF). CSF culture and blood culture were sterile. Empiric antimicrobial therapy with third generation cephalosporin and aminoglycoside was instituted. However, no improvement was observed. Patient expired four days after surgery due to increased intracranial pressure and tentorial herniation. Discussion This is the first case of S. apiospermum abscess encountered in this geographic area highlighting the involvement of fungal agent in brain abscess. Most case reports of S. apiospermum brain abscess have documented CSOM to be the risk factor as in this case. S. apiospermum is a filamentous fungus that is found worldwide. It has been isolated from soil sewage, contaminated water and the manure of farm animals. It has asexual and sexual reproduction. The asexual form is called Scedosporium apiospermum . Microscopically it produces golden brown elliptical single celled conidia borne singly from the tips of long or short conidiophores. P. boydii is the sexual form (teleomorph) of the organism. The sexual form exhibits cleistothecia, which are sac like structures that contain asci and ascospores. When the latter are fully developed the large thick walled cleistothecia rupture and liberate the asci and ascospores. The ascospores are oval delicately pointed at each end and resemble the conidia of the asexual form.[3],[4] Forty percent of brain abscesses are associated with otitis media or mastoiditis.[5] Neglect or delayed management of CSOM may lead to serious sequelae. Intracranial complication is a serious threat, as was seen in the present case.[5] Invasive infections have also been reported in patients receiving treatment with corticosteroids and immunosuppressive therapy for organ transplantation, leukaemia, lymphoma, systemic lupus erythematosus or Crohn′s disease. Infections include invasive sinusitis, pneumonia, arthritis with osteomyelitis, cutaneous and subcutaneous granulomata, meningitis, brain abscesses, endophthalmitis and disseminated systemic disease.[6] Disseminated and invasive infections with this organisms seen primarily in immunocompromised hosts include pneumonitis, osteomyelitis, endophthalmitis and prosthetic valve endocarditis. Central nervous system (CNS) scedosporiosis remains relatively rare. Central nervous system involvement has been reported in various world literature including cases of solitary or multiple brain abscesses, ventriculitis, meningitis.[4],[5] Central nervous system infections are notoriously difficult to treat are fatal in most cases.[7] High mortality rate of CNS infections may be due to delay in diagnosis and to the lack of effective agents that adequately penetrate the blood brain barrier. Early antifungal treatment in conjunction with surgical management may have had a better prognosis in our patient. Common antifungal drugs (amphotericin B, fluconazole, itraconazole) are variably active in vitro against S. apiospermum, CSF concentrations of these drugs are less than 1% of serum concentrations.[8] Therefore, these drugs are not very effective in treating the CNS infections by S. apiospermum . Voriconazole concentrations in the CSF are 50% of serum concentrations and reports of successful outcomes in patients with CNS infections treated with this agent are increasing. Currently, voriconazole seems to be the antifungal agent of choice for CNS infections caused by S. apiospermum .[9],[10] The present case highlights the importance of early diagnosis and documentation of rarely encountered S. apiospermum in CNS infection. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06067f1.jpg] |
| |||||||||
{kind=link}