 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
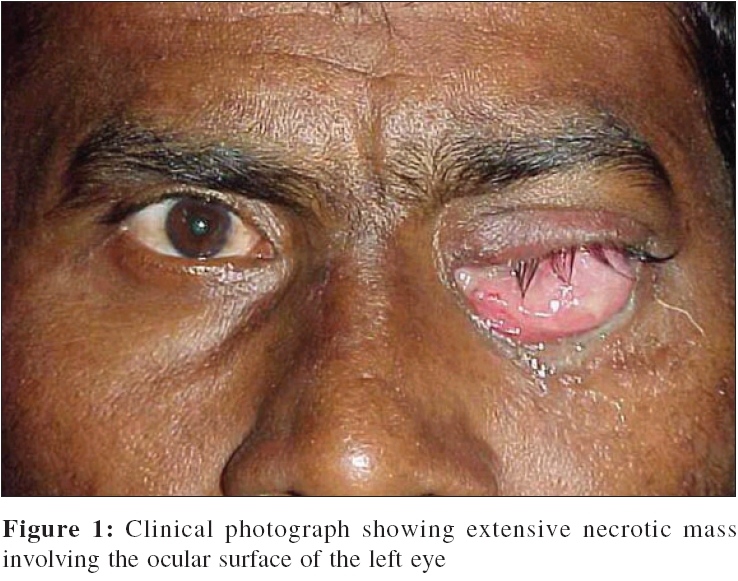
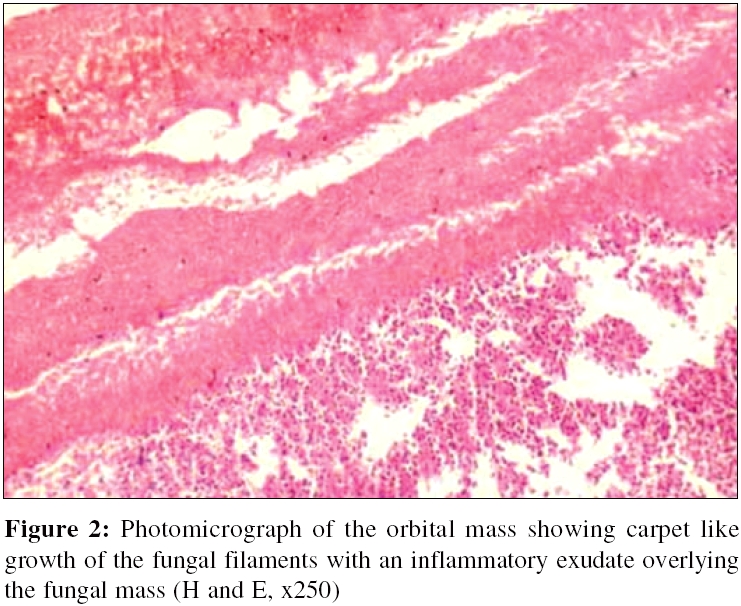
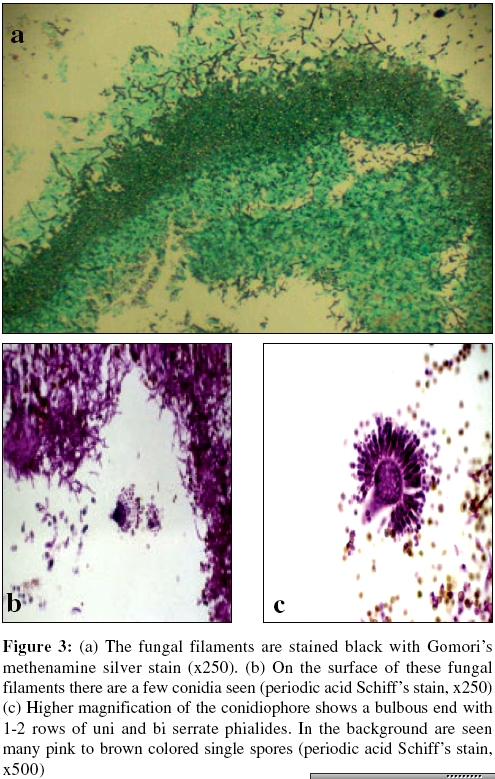
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 233-234 Case Report Primary orbital aspergilloma of the exenterated orbit in an immunocompromized patient Naik MN, Vemuganti GK, Honavar SG Ophthalmic Pathology Service, L.V. Prasad Eye Institute, L.V. Prasad Marg, Banjara Hills, Hyderabad - 500 034, Andhra Pradesh Code Number: mb06068 Abstract Aspergilloma is a fungal ball that usually forms in a preformed stationary cavity, mostly in lung and paranasal sinuses. We report a rare case of primary orbital Aspergilloma following exenteration for an invasive ocular surface squamous neoplasia, clinically mimicking a recurrence of the tumor. The fungal ball showed the presence of conidiophores with a globular head and a complete row of uni and biserrate phialides, suggestive of Aspergillus flavus species. The exposure to air in the orbit, possibly promoted the formation of conidiophores, which are normally seen when the organism is located in air cavities.Keywords: Aspergilloma, Orbit, Condiophores Aspergilloma is a fungal ball that usually forms in a preformed stationary cavity, as seen in lung and paranasal sinuses.[1] It can occur in the orbit by contiguous spread of sino-nasal aspergillosis,[2],[3],[4] rarely as a primary manifestation.[5],[6] We report a rare case of primary orbital aspergilloma following exenteration for an invasive ocular surface squamous neoplasia, which to the best of our knowledge has not been reported before. Clinically, this mass like lesion with rich vascular supply may mimic tumor recurrence. Case Report A 52- year- old male presented with the complaints of pain, watering, frequent bleeding with discharge and a rapidly increasing mass in the left eye since one month. Examination revealed abnormalities limited to the left eye, which had no light perception. Ocular examination of the left eye showed a necrotic mass covering the entire bulbar surface (Fig. 1). The eyeball could not be visualized. Regional lymph nodes were not palpable. Orbital CT scan showed intraocular as well as orbital extension into the medial orbit. The medial rectus muscle was thickened. The paranasal sinuses, however, appeared normal. Based on the above findings, the patient was diagnosed to have ocular surface squamous neoplasia (OSSN), with intraocular and orbital extension. Following histologic confirmation of the diagnosis by an incisional biopsy, the patient underwent lid-sparing exenteration of the left orbit and transverse blepharorraphy. The patient was found to be HIV positive. Two weeks later, he presented with wound dehiscence and purulent discharge (not cultured) in the exenterated socket, which responded to broad spectrum antibiotics within 10 days. Six weeks later, he presented with a pedunculated mass at the orbital apex measuring 10 x 5 mm. The mass was black and could be easily lifted from the bed that consisted of granulation tissue and blood clots. The excised mass was sent for histopathologic examination, with a clinical suspicion of either an orbital recurrence of the tumor or an organizing blood clot. The exenterated orbit was otherwise healthy and lined by granulation tissue. Histopathology demonstrated neutrophillic exudates over a thick sheet of septate and branching fungal filaments (Fig. 2). Many of the fungal filaments showed dilated ends, brownish discoloration of the walls. The fungal filaments and conidiophores stained black with Gomori′s methenamine silver stain (Fig. 3a) and bright magenta pink with Periodic acid Schiff′s stain (Fig. 3b). In addition there were a few conidiophores with elongated to globular heads containing a radiating row of 1- 2 phialides on the surface (Fig. 3c). Based on these findings, a histopathologic diagnosis of aspergilloma was made. Discussion Aspergillosis in a common primary or secondary fungal infection.[1] The pathologic response caused by this condition varies with the severity of the infection, local and systemic immunologic and physiologic state of the host. In an immunocompromised host it occurs in the form of cutaneous, sino-orbital, pulmonary, central nervous system or disseminated infection.[1],[2],[3] It can also be associated with local tissue damage or foreign body entry as occurs in eye, bone, burn wounds and prosthetic valves. Aspergillosis of the orbit is a rare disease usually caused by the continguous spread of opportunistic organism from the oropharynx or paranasal sinuses.[4] The ethmoidal and sphenoidal sinuses are the usual loci of infection. The onset of the disease is usually chronic and insidious in healthy patients, but can have a fulminant presentation in immuno-compromised patients. Our patient had infection of the orbital socket that responded to broad spectrum antibiotic therapy, but six weeks later presented with a brown orbital mass mimicking a tumor recurrence or an organized blood clot. In the absence of clinical signs of inflammation, an infective etiology was negated and hence the entire mass was submitted for histopathologic evaluation. Histologic evaluation revealed a classical fungal ball along with conidiophores. The conidiophores seen in this case had a globular head with a complete row of uni and biserrate phialides, suggestive of Aspergillus flavus species. The conidiophores are typically formed when the organism is exposed to air cavities as seen in lungs and paranasal sinuses. In summary, aspergilloma of the exenterated orbit is extremely rare and can mimic tumor recurrence. Exposure to air supports not only the hyphal form but also the sporulating form of Aspergillosis. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06068f1.jpg] [mb06068f3.jpg] [mb06068f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}