 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
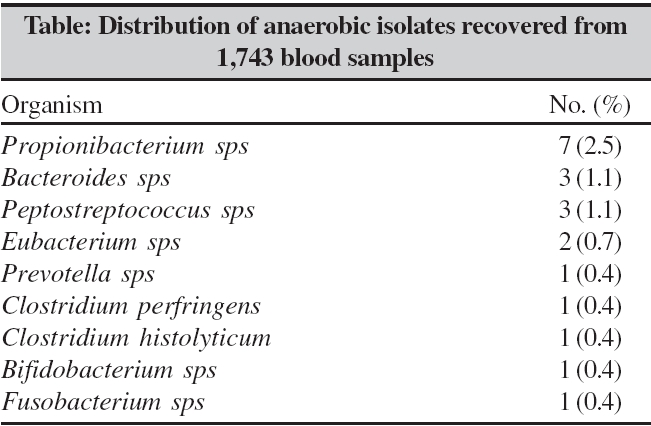
Indian Journal of Medical Microbiology, Vol. 24, No. 3, July-September, 2006, pp. 235-236 Correspondence Anaerobic bacteraemia in a tertiary care hospital of North India Singhal R, Chaudhry R, Dhawan B Department of Microbiology, All India Institute of Medical Sciences, New Delhi - 110 029Department of Microbiology, All India Institute of Medical Sciences, New Delhi - 110 029 Code Number: mb06069 Dear Editor, Anaerobic blood stream infections account for 0.5-12% of all positive blood cultures.[1] Different studies have given conflicting results about the incidence and clinical significance of anaerobic bacteremia.[1] This has created a doubt on the value of routinely performing anaerobic blood cultures by some investigators.[1] In Indian scenario, very few studies have been carried out to detect the rate of anaerobic bacteremia.[2] In the present study, we retrospectively reviewed the microbiological records of blood samples received for anaerobic culture during the period January 1992 to December 2002 at our hospital, which is a 3,000-bed tertiary care referral hospital of North India. A total of 1,743 blood samples were received in our laboratory. Anaerobes were identified by standard biochemical tests.[3] The anti microbial susceptibility testing and determination of MIC to metronidazole was done using E test strip (AB biodisk, Sweden).[3] All the strains were stocked. Identity of the stocked strains was reconfirmed by automated kits; Rap ID Ana II (Innovative diagnostic system, LP; Norcross, GA). A total of 299 bacterial isolates were obtained; of these, 20 (6.7% of all positive blood cultures) were anaerobes. Among 20 anaerobic isolates, 18 were isolated in pure culture and two isolates grew concomitantly with aerobes in two cultures. The table gives the distribution of 20 anaerobic isolates recovered from 1,743 blood samples. One strain of Bacteroides fragilis was found to be resistant to metronidazole with MIC of 256 mg/mL.[2] All the other isolated strains were found to be sensitive to metronidazole by disc diffusion test. The MIC of metronidazole against these strains was found to be in the range of 0.094 to 0.125 μg/mL. In the present study over ten years, the overall isolation rate of anaerobes in blood was found to be 1.2%. Another study has reported an isolation rate of 2.1%.[1] In our study, no significant decrease or increase in rate of anaerobic bacteremia was seen over a period of time. An England based study also did not find a change in the rate of anaerobic bacteremia over a ten-year period of 1969-79 and 1980-90.[4] This can be explained by the fact that the expected increase of isolation due to improved culture techniques is offset by the empirical treatment in recent times. Propionibacterium spp. were the commonest anaerobes isolated in our study unlike other studies.[5] Propionibacterium spp. have been traditionally considered as non-pathogenic in humans. However, its role as opportunistic pathogen is being increasingly recognized in variety of infections such as endocarditis, osteomyelitis, endophthalmitis, brain abscess and other debilitated state.[6] In the present study, all three Propionibacterium granulosum and one isolate of Propionibacterium acnes were considered significant because of their repeated isolation. Mortality associated with anaerobic bacteremia is high and reported to be in the range of 24 to 31% in most studies.[1],[3] In our study, the outcome in patients with metronidazole resistant Bacteroides fragilis , Clostridium histolyticum and Fusobacterium necrophorum was fatal.[2] Isolation of metronidazole resistant Bacteroides fragilis highlights the need for anti microbial susceptibility testing among all anaerobes. In conclusion, significant incidence of anaerobic bacteraemia, emerging antimicrobial resistance in anaerobes to commonly used anti microbials and high mortality rate necessitates the complete investigation of all blood cultures. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06069t1.jpg] |
| |||||||||
{kind=link}