 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
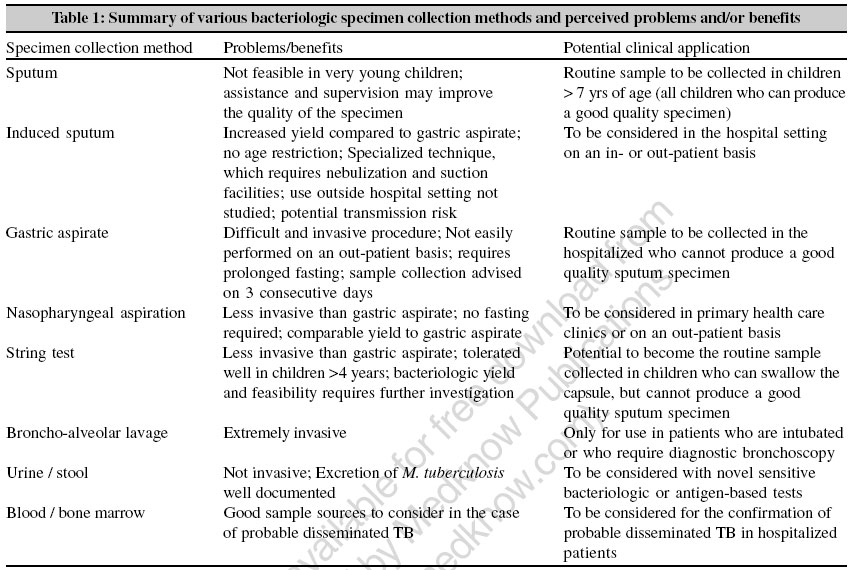
Indian Journal of Medical Microbiology, Vol. 24, No. 4, October-December, 2006, pp. 249-251 Guest Editorial Specimen collection methods in the diagnosis of childhood tuberculosis Marais BJ, Pai M Department of Epidemiology and Biostatistics, McGill University, Montreal Code Number: mb06074 The importance and severity of the childhood tuberculosis (TB) disease burden is recognized in many developing countries. Of the estimated 8.3 million new TB cases reported to the World Health Organization (WHO) in 2000, 884 019 (11%) were children.[1] However, the diagnosis of childhood TB is complicated by the absence of a practical gold standard, as bacteriologic confirmation is rarely achieved due to the predominantly paucibacillary nature of childhood TB.[2] Sputum microscopy, often the only test available in endemic areas, is positive in less than 10-15% of children with probable TB and culture yields are usually low (30-40%).[2] For this reason, in non-endemic areas, use of a diagnostic triad is widely advocated: 1) known contact with an adult index case (e.g., household contact), 2) a positive tuberculin skin test (TST) as evidence of M. tuberculosis infection and 3) suggestive signs on the chest radiograph (CXR).[2] However, accuracy of this triad is greatly diminished in developing countries where the majority of the population acquire infection during childhood and where transmission is not restricted to household contact with a known index case. Consequently, in endemic settings such as India where the discriminatory value of known M. tuberculosis exposure and/or infection is drastically reduced, the diagnosis of childhood TB depends mainly on clinical features and the subjective interpretation of the CXR. In such settings, there is a definite need to improve bacteriologic diagnosis of childhood TB and overcome the limitations of predominantly clinical approaches. Although the bacteriologic yield in children is low, adolescent children frequently develop sputum smear-positive adult-type disease and sputum microscopy has definite diagnostic value in this subset of children.[3] A recent study demonstrated that the bacteriologic yield in children with TB depends on the specific intra-thoracic manifestation of disease.[4] A yield of 77% was reported in children with advanced disease, while the yield in those with uncomplicated hilar adenopathy was only 35%, using the liquid broth MGIT® system (Beckton Dickinson, MD, USA). This observation demonstrates the potential value of traditional, as well as more advanced bacteriology-based diagnostic approaches, particularly in endemic areas such as India where children frequently present with advanced disease. Automated liquid broth cultures such as MGIT ® and BACTEC ® offer slightly superior sensitivity and reduced turn around time compared to the conventional solid media. However, their excessive cost and requirement for laboratory infrastructure remains a major limitation. Alternative, simple and rapid mechanisms for detecting mycobacterial growth (e.g., colorimetric cultures) have been developed, but require further validation in children.[5] Collection of bacteriologic specimens is a major challenge in the workup of a case of suspected pediatric TB. [Table - 1] shows various methods that are used to collect bacteriologic specimens, their limitations and potential advantages. Two to three fasting gastric aspirates collected on consecutive days and usually requiring hospital admission are routinely advised in children who cannot cough up sputum. A retrospective study from California compared the bacteriologic yield achieved in gastric aspirates collected from hospitalized and non-hospitalized children.[6] Although the yield in hospitalized children was higher (percentage of positive cultures 48% vs 37%), this difference was not statistically significant,[6] which suggests that hospitalization may not be a prerequisite for the collection of a good gastric aspirate specimen. Bronchoalveolar lavage, using flexible fiberoptic bronschoscopy, has additive value when used in combination with gastric lavage, but this technique is highly specialized and is unavailable in most endemic areas.[7] In a study from Peru, mid-morning nasopharyngeal aspiration was compared with early morning gastric aspiration; gastric aspiration provided a slightly better yield than nasopharyngeal aspiration (38% vs 30%), but the results were comparable.[8] Nasopharyngeal aspiration is minimally invasive, does not require hospitalization or fasting and can be performed at any time of the day. Sputum induction is another non-invasive approach. A South African study showed that a single specimen, using hypertonic-saline induced sputum collection, may provide the same yield as three gastric aspirate specimens.[9] However, the overall yield in this study remained poor (15% with one and 20% with three induced sputa), the technique has not been used outside the hospital setting and induction may pose a nosocomial exposure risk if the procedure is performed in a setting with no TB infection control systems in place. Additional studies are required to confirm the feasibility, safety and diagnostic value of collecting induced sputum specimens in primary health care settings. The string test is a novel approach that has recently been evaluated for its ability to retrieve M. tuberculosis .[10] This test, originally developed for the retrieval of enteric pathogens, consists of a coiled nylon string inside a gel capsule. The string unravels through a hole in the end of the weighted capsule as it descends into the stomach and the capsule then dissolves in the stomach. The unraveled string becomes coated with gastro-intestinal secretions and pathogens, if present, are retrieved when the string is extracted four hours later.[11] This test demonstrated superior sensitivity compared to induced sputum in sputum smear-negative HIV-infected adults with TB symptoms and was generally well-tolerated. A recent study showed that the string test is well-tolerated in children as young as four years.[11] However, there are currently no published data on the bacteriologic yield of this test in children. The most common extra-thoracic manifestation of TB in children is cervical lymphadenitis. Fine needle aspiration, using a small 23G needle, is a robust and simple technique with minimal side-effects that provides excellent diagnostic value.[12] Collection of blood specimens in children is a challenge, especially in infants. Blood draw may be indicated for performing serological assays for TB and for diagnosis of latent infection using interferon-gamma release assays (IGRAs). However, serological assays for detection of TB antibodies have been disappointing; no serological assay is accurate enough to replace conventional tests and they have no clinical role at present.[5] The development of antigen detection immunoassays may pave the way for blood-based diagnosis of active TB.[5] Although IGRAs are more specific than the TST for detection of latent TB infection,[13] they may have limited applicability in high burden countries such as India.[14] They are expensive and require laboratory infrastructure.[14] Also, there is lack of strong evidence on the clinical utility of IGRAs in children in tropical countries.[13] In India, research work on IGRAs,[15],[16] including a study among children,[17] has shown that the TST and a whole-blood IGRA produce comparable results and both tests are unaffected by previous BCG vaccination. The TST, therefore, continues to be a fairly useful test in the Indian context, especially in settings with limited laboratory capability. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06074t1.jpg] |
| |||||||||
{kind=link}