 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
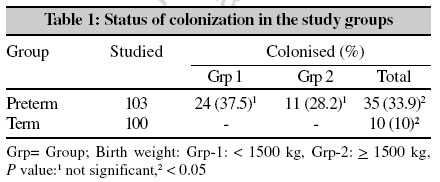
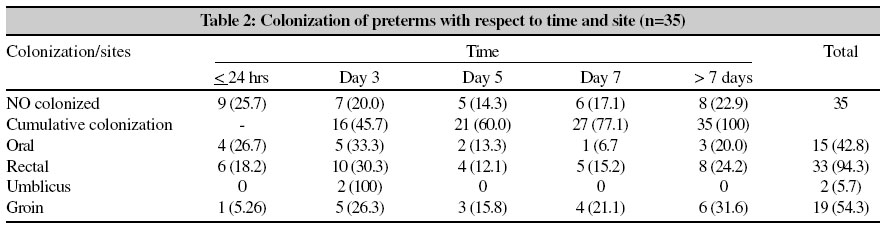
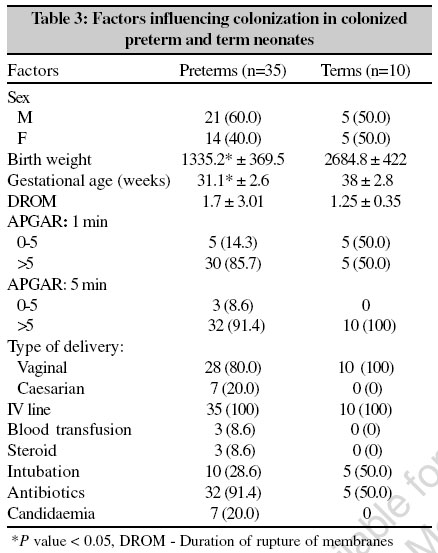
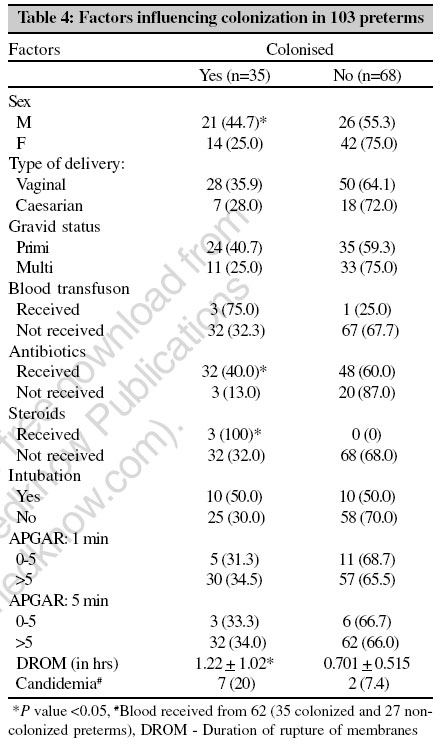
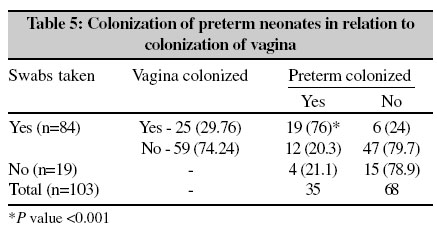
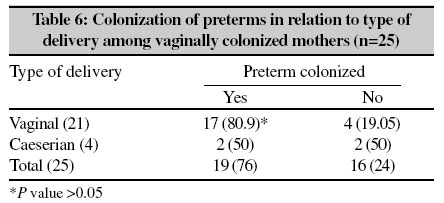
Indian Journal of Medical Microbiology, Vol. 24, No. 4, October-December, 2006, pp. 263-267 Original Article Candida colonization in preterm babies admitted to neonatal intensive care unit in the rural setting Mendiratta DK, Rawat V, Thamke D, Chaturvedi P, Chhabra S, Narang P Department of Microbiology, Mahatma Gandhi Institute of Medical Sciences, Sevagram - 442 102, Maharashtra Date of Submission: 18-Mar-2006 Code Number: mb06077 Abstract Purpose: Candida colonization in neonates results in significant morbidity and mortality. The purpose of this study was to determine colonization of Candida spp. in preterm babies and identify the risk factors.Methods: Swabs from oral, rectum, groin and umblicus of 103 preterm and 100 term neonates were obtained within 24 hours of birth, day three, day five, day seven and thereafter every week till the neonate was admitted in the neonatal intensive care unit (NICU). Swabs were also collected from the mother's vagina prior to delivery. Twice every month, air of the NICU was sampled by settle plate and swabs were collected from the hands of health care workers and inanimate objects of NICU. Identification and speciation was done by standard methods. Antibiotic sensitivity was studied against amphotericin B, ketoconazole and fluconazole by disk diffusion method. Results: Colonization with Candida was significantly higher in preterms. Earliest colonization was of oral mucosa and 77.1% of the preterms had colonised at various sites by the first week of life. Significant risk factors in colonized versus non-colonized preterms were male sex, longer duration of rupture of membranes (DROM), administration of steroids and antibiotics and vaginal colonization of mothers, whereas those in preterms versus terms were low birth weight and gestational age. C. albicans was the commonest species, both in the colonized preterms (45.9%) and vagina of mothers. Resistance was seen to fluconazole and ketoconazole only. No Candida spp. was isolated from health care personnel or environment. Conclusions: Colonization of preterms by Candida is a significant problem in NICU and the significant risk factors observed in colonized preterms were male sex, longer DROM, administration of steroids and antibiotics and vaginal colonization of mothers. Keywords: Candida, colonization, preterms Candida spp. are important nosocomial pathogens in the newborn population, particularly among the preterms. Colonization of the neonatal skin and gastrointestinal tract is the first step in the pathogenesis of invasive Candidiasis .[1] C. albicans is the most commonly isolated species in colonized or infected infants. However, in the past decade infection and colonization with other species of Candida has risen dramatically and high rates of yeast carriage in neonates, especially preterms has been reported by many workers.[2],[3],[4] This has been attributed to the advancement in technology, life support systems, relative immunodeficiencies in the preterms, high prevalence of hand carriage of Candida in health care workers,[5],[6] ability of Candida to survive on environmental surfaces[7] and colonization of maternal vagina.[8] Colonization of the infant occurs early in life and this is affected by a variety of common practices in the neonatal intensive care unit (NICU). Presently, there is a paucity of information on fungal colonisation in preterm infants. Keeping the above facts in view this study had been undertaken in preterms admitted in NICU of a rural tertiary care hospital to find out the rate, risk factors and source of colonization by various species of Candida . Materials and Methods Between August 2001 and September 2002, 142 preterms (born before 37 completed weeks of gestation) were admitted in the NICU of this rural hospital in Wardha district, Maharashtra state. Out of these, two died and 37 were discharged within few hours of admission. Hence, 103 preterms were included in the study. One hundred healthy term neonates were included as controls. Collection of specimens Swabs Swabs from oral, rectal, umbilical and groin area of 103 preterm neonates were collected within 24 hours of birth, day three, five, seven and thereafter every week till the neonate was admitted in the NICU. From term neonates swabs were collected within 24 hours. High vaginal swab from mothers was collected prior to delivery by the obstretician and transported to the laboratory within 30 minutes of collection. Vaginal swabs from 84 mothers of preterms could be collected. Swabs were taken from hands of all attending health care workers (doctors and nurses) twice a month during the study period. Swabs were also taken from washbasin (NICU - twice every month), cradle, blanket and incubaters of babies (only once, just before use by the neonate) Sterile cotton tipped swabs were used for collection after moistening them with sterile distilled water. On the day of collection swabs were collected from all the staff working in the shift of the collection day by rubbing the swab all over the palmar surface, fingers and webs of both the hands. Air of different areas of NICU was sampled by settle plates twice in the month during the study period. For air sampling, 90 mm diameter Sabourauds dextrose agar (SDA) plates were used. Four plates were placed in different areas of the NICU for 30 minutes each time. Collection of blood was not part of the study. Blood sent by the paediatrician as and when found necessary was processed. However, during the study period, whenever required, blood was collected by the paediatrician in Biphasic brain heart infusion broth (BBHI). All samples were processed within 30 minutes of collection. Swabs were inoculated on SDA (Hi-Media) slants with gentamicin 2 mg/dL and chloramphenicol 5 mg/dL. The slants were incubated at 37°C for seven days. All BBHI bottles were incubated at 37°C and tilted daily for subculture. Any growth obtained on SDA slopes, SDA plates and agar of blood culture bottle was processed for identification of yeast by standard technique.[9] Anti fungal susceptibility testing of all isolates was carried out by disk diffusion method [10] against fluconazole, amphotericin B and ketoconazole. In case of neonates, information about i) receipt of antibiotics, steroids, blood transfusion, ii) APGAR score, iii) intubation, iv) birth weight and in mothers i) gravid status, gestational week, type of delivery, duration of rupture of memberanes (DROM) was noted and recorded. Data was analyzed using Students "t" test, Chi-square test and Fisher′s exact test wherever necessary. Results Colonisation in preterms (33.9%) was significantly higher ( P < 0.05) than that in healthy term neonates (10%). The 103 preterms were divided into two groups [Table - 1] on the basis of birth weight (Group 1: < 1.5 kg and Group 2: > 1.5 kg). Colonisation of group 1 preterms was higher (37.5%) than group 2 (28.2%), however, this difference in colonization was not significant. Hence, further analysis was done on total preterms and not among these groups. Among the colonized neonates acqusition of yeast occurred in 25.7% within 24 hours and by day seven, 77.1% of preterms were colonized. The remaining 22.9% were colonized after seventh day of birth [Table - 2]. Site of colonization Colonisation at two sites was seen in 57.1% preterms, one in 25.7% and more than two in 17.1%. However, none of these differences were significant. Colonization was maximum in the rectum (94.3%) followed by groin (54.3%) oral mucosa (42.8%) and umbilicus (5.7%), however earliest colonization i.e., within 24 hours was that of oral mucosa (26.7%). Colonisation of oral mucosa, rectum and groin continued even after day seven. Risk factors Male sex, longer duration of rupture of membrane, administration of steroids and antibiotics were found to be significant risk factors in preterms with colonization when compared to those without colonization. However, these were gestational age and low birth weight for colonized preterms when compared to colonized terms [Table - 3][Table - 4]. C. albicans (45.9%) was the most common species isolated from preterms followed by C. glabrata and C. tropicalis (21.6% each) and C. parapsilosis (8.1%). Candida carriage in mother′s vaginal tract 25 (29.8%) mothers of preterms were colonized by Candida [Table - 5] and 15 of the Candida spp. isolated from the vagina of such mothers were similar to those isolated from their neonates. Colonisation in preterms born to vaginally colonized mothers (76%) was significantly higher than those born to non-colonized mothers (20.3%) ( P < 0.001) [Table - 5] and among colonized mothers it was more in preterms born vaginally (80.9%) as compared to those born by caesarian section (50%) ( P > 0.05) [Table - 6]. No yeast could be isolated from hands of staff, environment and inanimate objects. Blood was received from 62 preterms (35 colonized and 27 non-colonized). Development of candidaemia was higher in colonized (20%) as compared to non-colonized (7.4%) preterms [Table - 4] and seven (20%) of the 35 colonized preterms developed fungaemia as compared to none in the term [Table - 3]. Antifungal susceptibility Sensitivity testing was performed on 78 isolates. All isolates of a particular species from different sites of same patient showed similar sensitivity pattern . 40.3% of Candida strains isolated from the preterms were sensitive to all the three drugs (amphotercin B, fluconazole, ketokonazole). None of the isolates were resistant to amphotercin B. Resistance to fluconazole was seen only in C. albicans (18.9%) and to both fluconazole and ketoconazole in 10.4% ( C. albicans - 45.5%, C. tropicalis - 15.4%). Discussion Disseminated candidiasis is an important cause of morbidity and mortality in preterms and the first step in the pathogenesis of invasive Candidiasis disease is colonization.[1] Colonization by yeast among preterms in the present study was significantly higher (33.9%) than that observed in terms (10%). This may be because of relative immunodeficiency in preterms, such as decreased function of neutrophils and relative quantitative deficiency of protective maternal IgG to Candida.[11] The frequency of colonization observed in our study was close to that reported by Baley et al[4] (27%) and Sharp et al[2] (28.2%) as far as pretems are concerned and that with Kozin et al[12] in case of term neonates (10%). However, Singh et al[3] reported a higher rate (74.4%). Rate of colonization depends upon management protocol and nature and intensity of routine antifungal antiseptic measures applied in a particular set up,[2] hence the variation. It is generally recognized that colonization of newborn with Candida occurs in the first few hours of life.[2],[13] In the present study colonization occurred within 24 hours (25.7%) and oral colonization was the commonest amongest these babies (26.7%). Most of the babies in our study were colonized by day seven and maximum colonization was seen in rectum (94.3%) as also observed by others.[4],[14] Gastrointestinal or respiratory tract colonization predominantly occurs during the first week[2],[4] and the gastrointestinal tract can serve as a reservoir from where the fungus can spread, particularly if there is a breach in mucosal lining[15] and also due to poor local colonization resistance.[16] Significant risk factors observed in our study in preterms as compared to terms were low birth weight and gestational age [Table - 4], while that among colonized preterms they were male sex, prolonged DROM, administration of steroids and antibiotics [Table - 3] and vaginal colonization of mothers [Table - 5]. Prolonged DROM, especially in vaginally colonized mothers favours ascending infection or colonization. The facts that i) Isolates of Candida from preterms and vagina of their respective mothers were similar in species and antibiotic sensitivity pattern in fifteen of them, ii) colonization of preterms born vaginally in vaginally colonized mothers was significantly more ( P < 0.001, [Table - 5]) and iii) that the earliest colonization was that of the oral mucosa (probably aspiration during vaginal passage) showed that vaginal colonization / infection is an important risk factor for the colonization in neonates.[8],[13] Hence, i) mandatory screenning of all pregnant women for Candida , irrespective of symptoms and ii) treatment of all, irrespective of vaginal colonization or infection is necessary to prevent colonization and subsequent infection of the neonates, especially preterms. Steroids and antibiotics are known to suppress immune system[11] and their administration to already immunodeficient preterms promotes colonisation. The species of Candida colonizing the neonates in our study were similar to that reported by others[2],[3],[4] and the commonest was C. albicans (45.9%). In the present study none of the samples from NICU or from hands of health care workers were positive for Candida as also reported by Baley et al[4] and Burnie et al.[6] In contrast, a high yeast carriage by health care personnel of a tertiary care hospital in Chandigarh was considered to be the possible reason for high yeast colonization among preterms admitted in the NICU.[3] The antifungal sensitivity pattern of C. albicans isolated from blood and colonized site (rectum) was identical in seven preterms neonates in the present study, indicating the probable site of entry. Prior colonization of mucous membrane has been reported to be an important risk factor for candidemia by others also.[1],[3] To conclude, colonization of preterms by Candida is a problem and needs attention, especially in the patients with identified risk factors, to avoid their dissemination and causation of life threatening infections. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06077t5.jpg] [mb06077t4.jpg] [mb06077t3.jpg] [mb06077t2.jpg] [mb06077t1.jpg] [mb06077t6.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}