 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 4, October-December, 2006, pp. 280-282 Brief Communications Serodiagnosis of dengue virus infection in patients presenting to a tertiary care hospital Neeraja M, Lakshmi V, Teja VD, Umabala P, Subbalakshmi MV Department of Microbiology, Nizam's Institute of Medical Sciences, Punjagutta, Hyderabad - 500 082, Andhra Pradesh
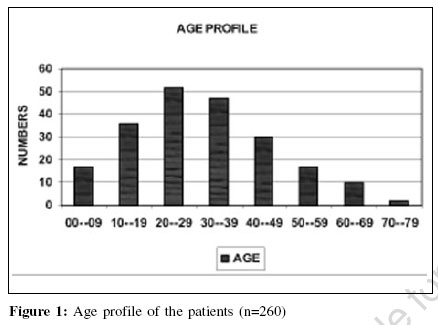
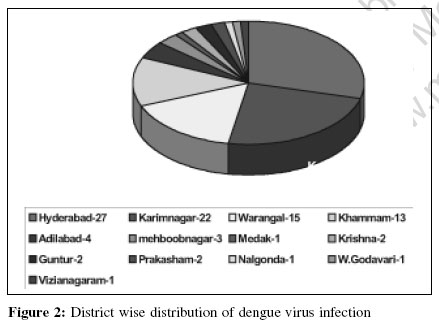
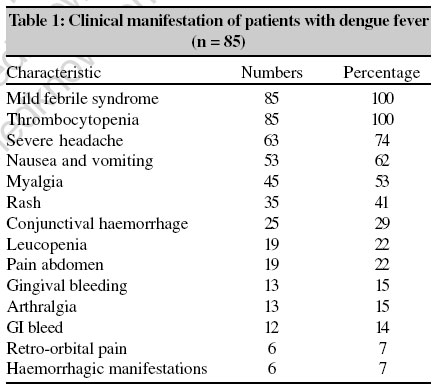
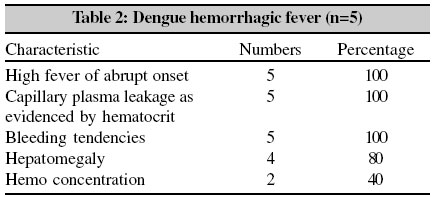
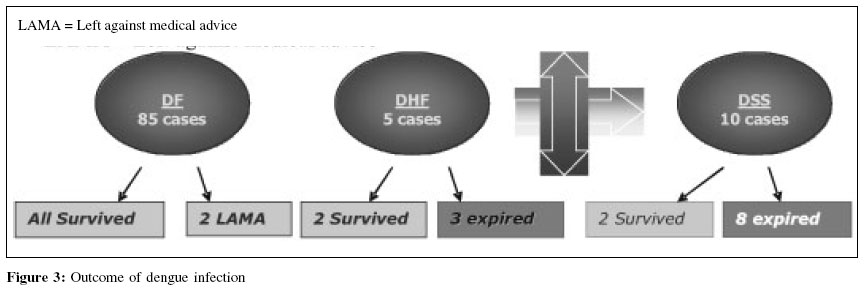
Date of Submission: 21-Oct-2005 Code Number: mb06080 Abstract Dengue is an acute infectious disease of viral etiology. It is probably one of the most important arthropod borne viral disease in terms of human morbidity and mortality. The spectrum of disease ranges from self-limited dengue fever to more severe forms of dengue hemorrhagic fever (DHF) or dengue shock syndrome (DSS). Laboratory diagnosis of dengue virus infection mainly depends on detection of virus specific antibodies. The aim of the study was to correlate the serological results with clinical presentation in patients with a diagnosis of dengue. Eleven out of 15 (73.3%) patients with DHF and DSS had secondary antibody response and mortality was 100% in these patients.Keywords: Dengue haemorrhagic fever, dengue shock syndrome, IgG, IgM, primary infection, secondary infection Dengue, also called classic dengue or break bone fever, is a flaviviral infection found in large areas of tropical and subtropical regions.[1] Dengue is a mosquito borne viral infection and is transmitted by Aedes aegypti and Aedes albopictus.[2],[3] Four distinct serotypes of viruses DEN-1, DEN-2, DEN-3 and DEN-4[3],[4] cause dengue. Humans are the main-amplifying hosts of the virus.[1] Dengue may be asymptomatic or may lead to undifferentiated fever, dengue fever (DF) or dengue hemorrhagic fever (DHF) and dengue shock syndrome.[5] DHF and dengue shock syndrome (DSS) are leading causes of hospitalization and death especially among children.[3],[6] The environmental risk factors for DHF are infestations with Aedes mosquito, hot and humid climates enhancing mosquito breeding, mosquito density and presence of all the four serotypes of dengue virus with secondary infection in the host, the water storage pattern in the houses, population density and large movement of people towards urban areas.[1] Early diagnosis of dengue is important and can be established with commercially available serological assays.[1] Early case detection and management reduce morbidity and mortality due to DHF or DSS. The main objective of this study was to evaluate the utility of serodiagnosis of dengue virus infection and correlate the results with demographic, clinical and laboratory profile in patients clinically diagnosed to be suffering from dengue at a tertiary care hospital in Hyderabad, Andhra Pradesh, South India. Materials and Methods During the period between September to December 2004, there was an outbreak of dengue in the city of Hyderabad and surrounding districts, in the state of Andhra Pradesh, South India. Two hundred and sixty patients suspected to be suffering from dengue fever /DHF/DSS were referred to our Institute. Serum collected from all the 260 patients were tested for IgG and IgM anti dengue antibodies by dengue IgG capture enzyme-linked immunosorbent assay (ELISA) and dengue IgM capture ELISA (PanBio Pty Ltd, Queensland, Australia). The dengue/DHF case investigation forms (WHO) were filled in by clinicians.[7] Case records of 100/211 seropositive patients who needed admission, were analyzed for demographic, clinical and laboratory data. The remaining 111 seropositive patients were managed on a conservative out-patient basis. As per the WHO classification, the proposed probable diagnosis - an acute febrile illness with two or more of the following manifestations - headache, retro-orbital pain, arthralgia, rash, haemorrhagic manifestations, leucopenia and a positive IgM antibody test on serum samples collected five or more days after the onset of fever supports the diagnosis of dengue.[5] A primary infection is indicated when the IgM to IgG index value ratio is 1.78 and secondary infection is indicated when the IgM to IgG ratio is less than 1.78.[8] Taking these criteria into account, patients have been categorized as suffering from primary/secondary infections. Results Two hundred and eleven of the 260 suspected cases of dengue were seropositive and 100 of these seropositive patients required admission. The age of the seropositive patients ranged between 9 to 78 years. The most affected age group was between 20 to 39 years. The male to female ratio of the seropositive patients was 2:1 [Figure - 1]. Since, our Institute is situated at Hyderabad in the Telangana region of Andhra Pradesh, most of the patients included in this study were referred from the surrounding districts in this region. Majority of the patients were from the city of Hyderabad, followed by Karimnagar, Warangal and Khammam [Figure - 2]. The major clinical findings in the reported DF cases were febrile illness, thrombocytopaenia, severe headache, nausea and vomiting [Table - 1]. In the five patients who progressed to DHF, the major clinical findings were abrupt onset of high fever, capillary plasma leakage and bleeding tendencies [Table - 2]. Ten patients progressed to DSS. They had persistent hypotension, rapid and weak pulse, restlessness, cold and clammy skin. Of the 211 sera, which gave positive results with IgG/IgM capture ELISA, IgG antibodies only were detected in 40.28% cases, IgM antibodies only in 3.8% cases and both IgG and IgM in 55.9% cases. Secondary dengue infections were more predominant (79%) in our series. On correlating the serological results with the clinical types of presentation of dengue among the study patients, 68/85 (80%) DF patients and 11/15 (73.3%) patients with DHF or DSS had a secondary antibody response. While all the 85 patients with uncomplicated DF survived, 3/5 (60%) patients with DHF and 8/10 (80%) patients with DSS expired. In all 11 of the expired patients there was a secondary antibody response with 100% mortality [Figure - 3]. Discussion The epidemiology of dengue in the Telangana region of Andhra Pradesh showed that most reported cases occurred in young adults. Our data shows that the epidemic waves were seen in urban centers, because highly urbanized areas have substantial proportions of the populations living in crowded impoverished areas with poor sanitation.[1] These complex urban settings are present in many regions in Hyderabad and surrounding districts posing a major challenge to vector control activities. Among the clinical signs, we noticed a higher proportion of febrile syndrome, thrombocytopaenia, severe headache, nausea, vomiting, myalgia and rash in patients with DF. DHF is a biphasic febrile illness, with hemorrhagic tendencies due to plasma leakage and increased vascular permeability.[5] Laboratory criteria for confirmation of dengue fever are isolation of dengue virus from serum and detection of dengue virus genomic sequences by polymerase chain reaction.[9] However, these tests are available only in reference laboratories and not available routinely. Hence, serological tests that demonstrate a fourfold or greater rise in reciprocal IgG or IgM antibody titre to one or more dengue virus antigens in the serum have greatly enhanced our ability to effectively and efficiently diagnose dengue infections. The serological tests using IgM capture and IgG capture ELISA in which the cut off value of the IgG is set to discriminate between high levels of IgG (characteristic of secondary dengue infections) and lower IgG (characteristic of primary /past dengue).[10] With this method, a majority of secondary dengue infections could be clearly delineated. Quantitation of antidengue IgG in these tests allows distinction between primary and secondary infections. In this study, 153/211(72.5%) showed secondary serological response and was more predominant among all the types of dengue. High mortality in the DHF/DSS cases with secondary response indicates that emphasis is needed for a close monitoring and conservative management to reduce morbidity and mortality. In spite of best treatment given to DSS patients, they succumbed to the infection because of late presentation of these patients to the hospital. The DSS patients were already in shock during their presentation to the hospital and in spite of adequate fluids and supportive therapy given, they could not be revived. Among the patients who expired with DHF and DSS, secondary infections were observed, indicating the need for their conservative management to decrease the incidence of deaths. In our study, early serodiagnosis and admission of suspected dengue cases and prompt administration of intravenous fluids to individuals showing signs of premonitory vascular collapse have brought case fatality rates down sharply in dengue endemic areas. We believe that serological diagnosis has a role in categorizing primary and secondary dengue and it also serves as a predictor of disease progression and mortality especially in the severe forms (DHF and DSS). References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06080f1.jpg] [mb06080f2.jpg] [mb06080f3.jpg] [mb06080t2.jpg] [mb06080t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}