 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 4, October-December, 2006, pp. 286-288 Case Report Infective endocarditis due to brucella Purwar S, Metgud SC, Darshan A, Mutnal MB, Nagmoti MB Department of Microbiology, JN Medical College, Belgaum - 590 010, Karnataka
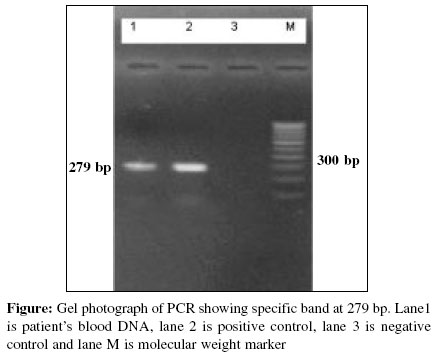
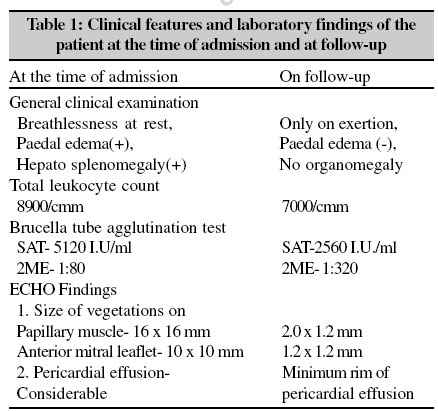
Date of Submission: 23-Aug-2005 Code Number: mb06082 Abstract One of the complications of brucellosis is infective endocarditis, which carries a high mortality rate if undiagnosed or misdiagnosed. We report a case of Brucella infective endocarditis, which was diagnosed serologically and by polymerase chain reaction. After Brucella specific treatment, patient showed dramatic improvement clinically, as evident by echocardiogram findings and other investigations.Keywords: Brucella, endocarditis, polymerase chain reaction Brucella infection is a zoonosis and the organism most commonly implicated is Brucella melitensis which is found in the Mediterranean, the Arabian Gulf, Latin America, Asia, parts of Mexico and the Indian sub continent. Brucellosis continues to be of great health significance and economic importance in many countries. No data is available about its prevalence in India but various studies conducted by different authors have reported the seropositivity ranging from 0.8% in general population to 58-72% in occupationally exposed personnel like veterinarians.[1] In humans, brucellosis behaves as a systemic infection with a very heterogeneous clinical spectrum. The disease usually presents as fever with no apparent focus, although in 20 to 40% of the cases there are focal forms. These focal forms of brucellosis have been described in almost all organs and systems, with the osteo articular forms being more common and those affecting the heart and the central nervous system being more severe. Cardiovascular complications of Brucellosis include endocarditis, myocarditis, pericarditis, aortic root abscess, thrombophlebitis with pulmonary aneurysm and pulmonary embolism.[2] Endocarditis and cardiac failure is a leading cause of mortality in 3-5% of cases. Brucella endocarditis may develop on valves, previously damaged by rheumatic fever or congenitally malformed, but may also occur on previously normal valves. The clinical features are indistinguishable from those of endocarditis caused by other organisms. High degree of suspicion, especially in susceptible population is essential for early diagnosis of Brucellosis and its complications, one of them being infective endocarditis. Case Report A male patient, aged 20 years, was admitted to the medical ward, in the department of medicine of KLE Hospital and Medical Research Center with complaints of intermittent fever with chills and rigors for a month and cardiac discomfort for last six months. The patient was a student and gave history of consuming raw milk and assisting in delivery of cattle at home since childhood (handling of afterbirths with bare hands). On examination, the patient was found to be breathless at rest, with pedal edema, tender hepatomegaly, pulsatile precordium, JVP raised and murmurs of MR and AR. On investigation, significant findings in the patient were: Haemogram-within normal limits, except raised total leukocyte count (8900/cmm). QBC for malarial parasite, Widal test and ASLO were negative. Brucella slide agglutination test was positive, Brucella standard tube agglutination test titers - 5120I U/ml and 2ME- 1:80. Polymerase chain reaction (PCR) was positive for Brucella melitensis [Figure - 1] and blood culture was negative after incubation till 30 days. Echocardiogram showed vegetations of 16 x 16 mm on papillary muscles and 10 x 10 mm on anterior mitral leaflet with pericardial effusion and severe AR and MR. Patient was put on WHO regimen for treatment of brucellosis consisting of rifampicin, doxycycline and streptomycin for 45 days and then reviewed on follow up. Significant improvement was observed in general condition of the patient which was substantiated by investigations [Table - 1]. Breathlessness and palpitation were only on exertion. There was no edema, no organomegaly and no murmurs. Investigations on follow up revealed significant improvement: Total leukocyte count was 7000/cmm compared to 8900/cmm, Brucella tube agglutination test titers - 2560 IU/ml, 2ME- 1:320 and Echocardiogram showed vegetations of 2.0 x 1.2 mm (compared to of 16 x 16 mm at the time of admission) on papillary muscles and of 1.2 x 1.2 mm (compared to 10 x 10 mm at the time of admission) on anterior mitral leaflet. Severe AR, moderate MR and minimal rim of pericardial effusion was observed. Patient improved clinically following the treatment and this improvement was evident on clinical examination and supported by ECHO findings, serology and haemogram. Blood culture being negative, diagnosis was confirmed by PCR, using Brucella melitensis specific primers. High titers of IgM component coupled with IgG in serology indicated acute exacerbation of chronic infection, which coupled with PCR results, history of persistent exposure and excellent response to Brucella specific therapy helped us to diagnose this case as infective endocarditis caused by Brucella . Because of early detection and specific therapy this patient had a good clinical outcome. Discussion Other authors have reported similar cases of Brucella infective endocarditis[3],[4] from different parts of the world including Asia, Middle East and Latin America where it is still endemic.[5] Increased diagnostic and therapeutic vigilance is required for timely and efficient treatment of Brucella endocarditis. Diagnostically, high degree of suspicion is required, especially in patients with cardiac symptoms with a history of consumption of non-pasteurized dairy products, occupation associated with animal breeding or simply of living in rural areas. About half a million cases of brucellosis have been reported world wide, though detection rate varies around 30-40% of actual incidence.[6] Although Brucella endocarditis is a rare entity, it is associated with high mortality rates, hence high degree of suspicion is essential, specially in endemic areas. Serology plays a very important role in diagnosis of brucellosis for its ease of performance with good specificity and sensitivity.[7] Culture, though considered as gold standard, is not being always positive, isolation rates varying from 20 to 50% and may take up to one month and molecular techniques like PCR, though sensitive and specific,[8] are not available at all places due to limitation of resources. We are of the opinion that all sera from febrile patients should be screened for Brucella antibodies, as it does not cost much. If Brucella slide agglutination test is positive, it should be followed by standard tube agglutination test. It is suggested that the serum sample tested positive may also be subjected for modified SAT with 2 ME to distinguish between acute and chronic infection by knowing IgM and IgG components of total titers. This is especially important in endemic areas, because of presence of basal titers. Large number of samples can be screened quickly. In our institute we follow this policy and report almost two cases per month, most of which are not suspected by clinicians. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06082t1.jpg] [mb06082f1.jpg] |
| |||||||||
{kind=link}
{kind=link}