 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 24, No. 4, October-December, 2006, pp. 289-291 Case Report Necrotizing (malignant) otitis externa: An unusual localization of mucormycosis Tuzcu A, Bahceci M, Celen MK, Kilinc N, Ozmen S Department of Infectious Diseases, Diyarbakir
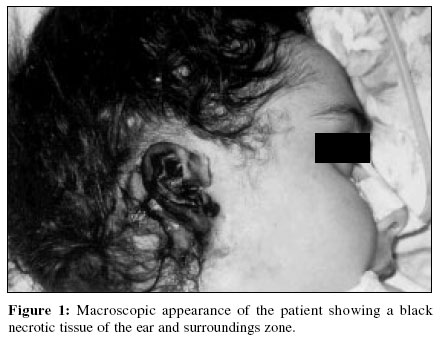
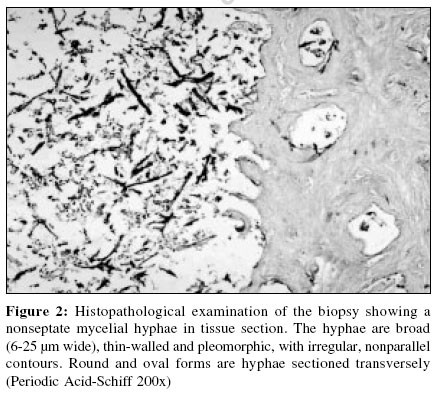
Date of Submission: 24-Apr-2006 Code Number: mb06083 Abstract Malignant otitis externa (MOE) is a severe infection of external auditory canal and skull base. A 17-year-old diabetic girl was admitted with diabetic ketoacidosis. Cellulitis of her right ear occurred on the second day of hospitalization and a black necrotic scar in the same region appeared on the next day. The lesion rapidly invaded to right side of neck and surrounding tissue of the patient. Therefore, antimycotic therapy was started. Unfortunately the patient died on seventh day of hospitalization because of probably extensive fungal invasion. Physicians should suspect MOE connected to mucormycosis especially in patients with cutaneous lesions of ear unresponsive to antibiotic therapy.Keywords: Mucormycosis, nonliposomal amphotericin B, unusual localization Malignant otitis externa (MOE) is a severe infection of the external auditory canal and skull base which most often affects elderly patients with diabetes mellitus. Early diagnosis and aggressive treatment are important in order to reduce risk of dissemination. Fungal MOE was first described in a granulocytopenic patient with acute myelogenous leukemia by Petrak et al .[1] Yao et al[2] described a patient with fungal MOE infection due to Scedosporium apiospermum , which had only been reported twice previously. Primary cutaneous mucormycosis is a considerably rare fungal infection, noted most often in immunosuppressed individuals. Although rhinocerebral mucormycosis is the most common form, primary cutaneous, pulmonary or gastrointestinal lesions may also develop and haematogenous dissemination to other sites can occur. Mucormycosis is the common name given to clinical disease caused by zygomycetes of the family Mucoraceae and the genera Rhizopus , Absidia and Mucor . The predisposing factors include diabetic ketoacidosis, immunosuppressive therapy, leukaemia, malnutrition, end-stage renal failure, severe diarrhoea and desferoxamine therapy. Patients without an underlying disorder or apparent predispositions have been also reported.[3] We report a fungal MOE infection with Mucoraceae in a female diabetic patient with diabetic ketoacidosis. Case Report A 17-year-old girl with de novo diabetes was admitted to the endocrinology department with diabetic ketoacidosis. Physical examination revealed a temperature of 38°C, a pulse of 112/minute, a respiratory rate of 24/minute and a blood pressure of 115/85 mm-Hg. The patient was unconscious. Arterial blood gas values demonstrated metabolic acidosis (pH: 6.9). Laboratory results were as follows; leukocyte: 28x10 3 /mm 3, haematocrit: 30%, ESR: 124 mm/hour. Plasma glucose: 25 mmol/L, BUN: 34 mg/dL, creatinine: 0.9 mg/dL, Na+: 128 mmol/L, K+: 4.3 mmol/L, AST: 38 U/L, ALT: 30 U/L, C reactive protein: 128 mg/dL, glycosuria (1000 mg/dL) and ketonuria (150 mg/dL) were detected in urine analysis. The urine culture was negative. Electrocardiogram and chest X-ray were found to be normal. Cellulitis of her right external ear occurred on the second day of hospitalization and a black necrotic scar in the same region appeared on the next day [Figure - 1]. It developed at the site, where a break in integrity of skin, as a result of trauma by bandage, used to keep endotracheal tube in a stable position during intubation. This lesion rapidly invaded to right side of neck and surrounding tissue of the patient. Clinically, this lesion was considered mucormycosis and antimycotic therapy was started with nonliposomal amphotericin B (Fungizone) at a dose of 2.0 mg/ kg/day intravenously. One day later amphotericin B dose was increased to 4 mg/kg/day and necrotic tissue was excised widely. Biopsy specimen was sent out for both pathological examination and microbiological study. Computerized tomography revealed inflammatory tissue changes occupying the right auricula and right side of his neck. Facial nerve paralysis occurred on the fifth day of hospitalization. Due to progression of lesions, the patient underwent surgery intervention again. Extensive debridement of right ear and related tissues was performed. In biopsy specimen, large, broad, nonseptate mycelial hyphae with right angle branching were observed [Figure - 2]. The sample was also inoculated onto blood agar, MacConkey′s agar and Sabouraud dextrose agar. Potassium hydroxide preparation showed broad, ribbon-like, aseptate hyphae when examined under a fluorescence microscope. On sixth day microbiology and pathology results from her ear specimen revealed Absidia corymbifera , a zygomycete. amphotericin B is replaced by liposomal complex form (ambisome) at the dose of 5 mg/kg. Despite all efforts diabetic ketoacidosis and fungal infection could not be controlled with regular insulin fluid replacement and liposomal amphotericin B. The patient died on seventh day of hospitalization because of probably extensive fungal invasion into the mastoid bone, cerebral vessels and brain parenchyma. Discussion Mucormycosis (zygomycosis) is an opportunistic fungal infection caused by fungi of the class zygomycetes order mucorales. In our patient, the microbiology results of sample revealed Absidia corymbifera , a zygomycete. It usually affects hosts compromised by underlying haematologic cancer, renal failure, immunosuppressive therapy, diabetes mellitus or burns and patients receiving desferoxamine.[4] More than 75% of the cases are those suffering from acidosis, especially diabetic ketoacidosis. One characteristic feature is that the blood vessels are flooded with fungus, which results in thrombosis, infarction and emboli. Acidosis disrupts iron binding of transferrin, resulting in increased proportion of unbound iron, which may promote growth of the fungus. Susceptibility of the patients with diabetic ketoacidosis to this infection may also be due to decreased neutrophil chemotaxis and phagocytosis. Diabetic ketoacidosis had made our patient prone to this progressive infection which is rare in normal hosts.[5] The presence of a black scar at the site of a previous bandage in our case was the first clue to the diagnosis of cutaneous zygomycosis. Mucormycosis lesions in the head and neck are most likely to occur in the nasal cavity and paranasal sinuses. The head and neck area is involved in only 14% of cutaneous cases. Of note, when cutaneous infections involve central structures (e.g, the head and neck), they have been associated with higher mortality than cutaneous infections limited to the extremities.[6] Although the unusual site of infection in our patient did not delay the diagnosis, the patient died despite antifungal treatment, similar with another previously reported otocerebral mucormycosis case.[7] Unique involvement of the middle ear, with facial paralysis has been reported in only one case previously.[8] In our case facial paralysis was detected in course of the disease which was probably reflecting middle ear involvement. Early biopsy of cutaneous mucormycosis lesions is imperative for optimizing outcome, as the infection can progress very rapidly. Biopsy and culture for bacteria and fungi are required to differentiate these lesions. Deep biopsies are necessary to diagnose the fungus. Superficial scrapings may only show necrotic tissue. The specimen should then be divided and one half send to the microbiology laboratory and the remainder send for histopathological evaluation.[9] Prior to the availability of amphotericin, mucormycosis was almost universally fatal. With earlier diagnosis and a combination of amphotericin and radical debridement of infected tissues, the fatality rate has dropped. In cases of diabetes, serum glucose levels must be regulated.[10] Debridement should be started as early as possible when the gangrenous form of the infection is detected. Liposomal amphotericin B has been used successfully.[10] Other antifungal agents such as fluconazole and miconazole are also used to treat mucormycosis. The management of this disease demands a multidisciplinary approach. Physicians should be alert with high index of suspicion of MOE due to mucormycosis in patients with cutaneous lesions of the ear that do not heal or are unresponsive to antibiotic therapy, especially in immunocompromised host. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06083f2.jpg] [mb06083f1.jpg] |
| |||||||||
{kind=link}
{kind=link}