 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
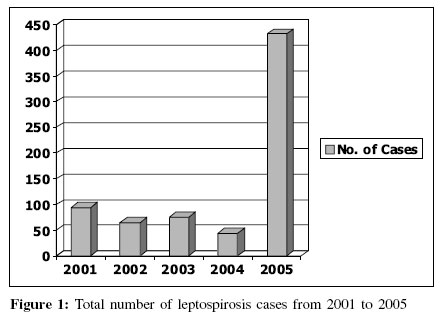
Indian Journal of Medical Microbiology, Vol. 24, No. 4, October-December, 2006, pp. 337-338 Supplement Leptospirosis in Mumbai: Post-deluge outbreak 2005 Maskey M, Shastri JS, Saraswathi K, Surpam R, Vaidya N Department of Microbiology, Topiwala National Medical College and BYL Nair Ch Hospital, Mumbai Code Number: mb06106 Leptospirosis is a worldwide zoonosis caused by pathogenic Leptospira spp. Humans are accidental hosts and can become infected through contact with an environment contaminated by the urine of a shedder host, such as a rodent. In tropical and subtropical regions, the disease is endemic and exposure to infection is widespread.[1] In India, leptospirosis is endemic in most of the urban areas, where epidemic outbreaks occur after flooding caused by heavy seasonal rainfall.[2],[3] The severity of this acute febrile illness varies considerably from mild to rapidly fatal. The wide spectrum of symptoms and signs makes clinical diagnosis very unreliable. Leptospirosis is frequently under-diagnosed, due to non-specific symptoms early in the course of the disease and the difficulty of performing both, the culture and microscopic agglutination test (MAT), the reference serological test, which require experienced personnel. To overcome this problem, some potentially useful screening tests for the use in all routine laboratories have been proposed.[4],[5] Serology plays a pivotal role in the early diagnosis of leptospirosis. In this study, we evaluated the diagnostic tests for leptospirosis on patients in Mumbai. Mumbai, the financial capital of the country experienced incessant rains (944 mm in 24 hours) on 26th July 2005, causing floods and subsequent water-logging. A large number of patients with fever came to the Nair hospital, a tertiary care center and the attached Infectious Diseases Hospital, the largest Infectious Diseases Hospital in South-East Asia. We also compared the prevalence of this disease over a period of five years as this acute febrile illness is widely recognized as a re-emergent disease.[6] Materials and Methods 1359 serum samples were obtained from patients admitted to the Nair Hospital and the Kasturba Hospital. These patients had history and clinical manifestations suggestive of leptospirosis, such as fever, anorexia, high-colored urine, conjunctival suffusion and decreased urine output. All the samples were screened by rapid tests/enzyme-linked immunosorbent assay (ELISA) tests. Rapid tests Rapid tests used were Leptotek Dri-dot, Leptocheck WB and Leptostix. ELISA The kit used was Pan-Bio Leptospira IgM ELISA. Another kit used was IgM Microwell ELISA using L. biflexa Patoc I (serovar Patoc) as antigen. The results were interpreted as per the manufacturers′ guidelines. MAT Paired serum samples obtained from 49 patients were sent to BJ Medical College, Pune, for confirmation by MAT. The serovars used were Australis, Bataviae, Icterohaemorrhagiae, Hebdomadis, Pomona, Tarassovi, Canicola and Autumnalis. Results Prevalence of leptospirosis during July, August and September in the years 2001-2005 was compared and a 8-fold rise in the year 2005 was observed [Figure - 1]. The 432 positive cases in 2005 were diagnosed either by rapid tests / ELISA subject to availability. The results on the 49 paired serum samples showed that all of them were positive by Lepto Dri-dot, 47 were positive by Panbio ELISA and only 24 were positive by MAT. Various studies have compared MAT, the reference test for leptospirosis, the Lepto Dri-dot assay and have shown an overall sensitivity of 90% and specificity of 92%.[7] Panbio Leptospira IgM ELISA has a sensitivity of 100% and a specificity of 95%.[8] Our study reveals the conformance of Screening tests with MAT as 48.97% in 2005 and 86% in the year 2004. The various serovars identified in the year 2005 were Icterohaemorrhagiae (13), Bataviae (10), Tarassovi (4), Canicola (2), Australis (1) and Pomona (1). In the year 2004, the serovars predominant were Canicola (17), Icterohaemorrhagiae (13), Australis (7), Pomona (3) and Pyrogenes (3). Icterohaemorrhagiae and Tarassovi were identified in two samples, which were negative by ELISA and positive both by rapid tests and MAT. Discussion The diagnosis of leptospirosis is often unconfirmed because of the lack of clinical suspicion, inappropriate sample collection and unavailability of testing facilities or a combination of these factors.[9] Serology plays a pivotal role in the early diagnosis of leptospirosis. Though MAT is the most widely used reference test, it has many limitations.[5] It is time-consuming and needs specialised personnel for its execution and the laboratory has to maintain strains for the preparation of live antigens. Knowledge of the prevalent serovars in a particular geographic area is required, as otherwise it would be cumbersome to test more than 200 serovars of L. interrogans and over 60 serovars of L. biflexa , especially in the situation of an outbreak. Examination of a large number of serum specimens during a situation of an outbreak may also compromise the quality of the results. Thus, there is an urgent need for a highly sensitive and specific test for early diagnosis of leptospirosis. Several rapid assays have been developed recently,[7],[9] which can be used for the screening of acutely ill patients. The sensitivity of these tests ranges from 96.5 to 100% and specificity from 95 to 99.8%.[7],[8] These tests are simple to perform, require minimum equipment and their interpretation is easy, curtailing technical expertise. As many of these tests have inbuilt controls, they are economical for single sample testing. When large numbers of samples need to be tested, conventional ELISA was preferred. In our observations in Mumbai in 2005, there was an eight-fold rise in the number of cases during August 2005 after heavy rainfall and water-logging. A significant finding was a sharp decline in the conformance of rapid/ELISA vis-à-vis MAT, as compared to the previous year. The various reasons for this could be inappropriate timing of sample collection, unavailability of paired sera and a restricted number of serovars used for confirmation. It was possible that new serovars were seen in this outbreak. As the prevalent serovars in this geographic area has not been determined and leptospirosis is endemic in the city of Mumbai, a detailed study is required. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06106f1.jpg] |
| |||||||||
{kind=link}