 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
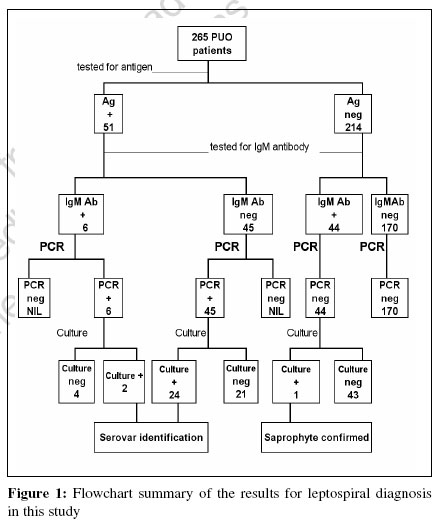
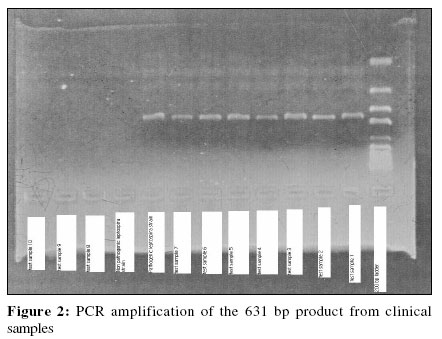
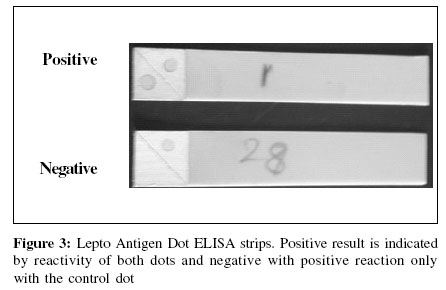
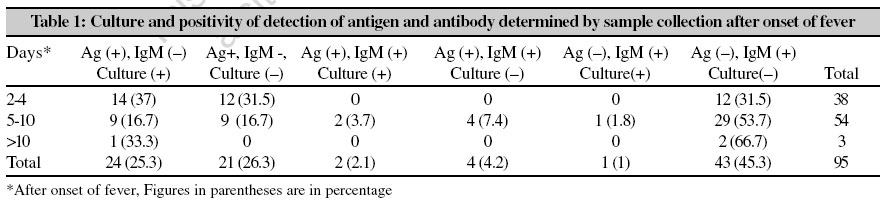
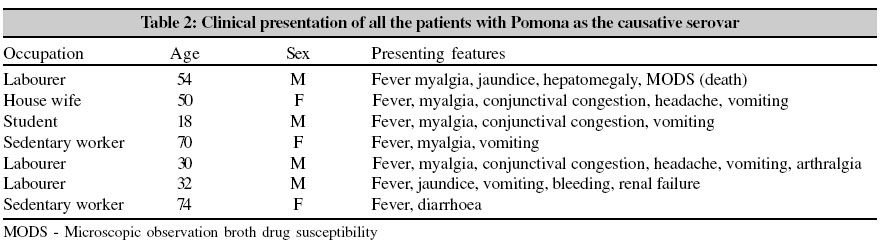
Indian Journal of Medical Microbiology, Vol. 24, No. 4, October-December, 2006, pp. 342-345 Supplement Early diagnosis of human leptospirosis by antigen detection in blood Nizamuddin M, Tuteja U, Shukla J, Nair L, Sudarsana J Department of Microbiology, Calicut Medical College, Kerala Code Number: mb06108 Leptospirosis is a zoonosis with multisystem involvement caused by the pathogenic strains of Leptospira spp. that affects humans and animals. It is considered to be the most widespread zoonotic disease in the world. Leptospirosis occurs as epidemic as well as sporadic outbreaks.[1] Leptospirosis is a disease of the environment; transmission depends on interactions between humans and mammalian reservoir hosts.[2] Animals may serve as carriers thus transmitting the disease while in humans the disease is usually acute that can result in severe or fatal disease.[3] Taylor and Goyal reported the first case of leptospirosis from India in 1929 from Andaman and Nicobar Islands.[4] There has been a significant increase in the reported cases of leptospirosis from India since 1980s. Epidemics have been increasingly reported from Orissa, Maharashtra, Karnataka, Tamil Nadu and Kerala. In Kerala, it is colloquially called Elippani (rat fever). The high prevalence of leptospiral infection of cattle represents potential threats to human health and agricultural economics.[5] Calicut Medical College caters to the need of Kozhikode district and adjacent districts and covers a population of more than eight million. People living in the rural area have contact with livestock and cattle. Epidemics of leptospirosis occur in monsoon seasons. The present study was done on early diagnosis of leptospirosis during the period July 2003 to December 2003, a period when there is the usual pattern of heavy rainfall. Materials and Methods Human patients 265 patients, visiting the out-patient department of Calicut Medical College from July 2003 to December 2003, inclusive of all age-groups and occupation-groups, consisting of agricultural workers, manual laborers, housewives, students and office workers were included in the study. Patients had symptoms of fever and myalgia with headache, vomiting, jaundice, conjunctival suffusion and abdominal symptoms. Blood Culture Fresh blood samples were collected from all antigen positive and antibody positive patients and EMJH medium was inoculated and incubated at room temperature for four to six weeks. Leptospiral antigen and antibody detection tests All the serum samples were tested for IgM antibody by PanBio IgM ELISA kit. Diagnostic kits, based on the principle of sandwich enzyme-linked immunosorbent assay (ELISA) were provided by Microbiology division, Defence Research and Development Establishment, (DRDE) Gwalior. This consisted of a microtitre plate coated with polyclonal leptospiral antibody, upon which theantigen capture was bound by the second antibody that consisted of a group of monoclonal antibodies specific for pathogenic strains of Leptospira spp. This consisted of monoclonal antibodies against the following serovars- Australis, Autumnalis, Bataviae, Canicola, Grippotyphosa, Hebdomadis, Icteroicterohaemorrhagia, Pomona, Tarassovi and Grippotyphosa + Hardjo. Detection was done by rabbit anti-mouse peroxidase conjugate, using ortho-phenylenediamine hydrochloride and hydrogen peroxide as substrate. The antigen detection was also devised as Dot ELISA strips. Nitrocellulose strips, coated with both control and polyclonal leptospiral antibody were used for detection. Polymerase chain reaction (PCR) analysis Serum was centrifuged and DNA was extracted from the pellet, using QIA DNA extraction kit. Polymerase chain reaction (PCR) was done using Hookey′s primers P1 - 5′ CGC TGG CGG CGC GTC TTA AA 3′ (20 mer) P2 - 5′ TTC ACC GCT ACA CCT GGA A 3′ (19mer) The PCR products were analysed on a 0.8% agarose gel Serovar identification of clinical isolates. The clinical isolates obtained from blood cultures were killed by keeping in a boiling water bath for three minutes and tested with a panel of serovar- specific monoclonal antibodies, using protocol as for antigen detection. Results The [Figure - 1] summarizes the results of the tests performed with the blood samples from 265 patients. Leptospiral antigen was detected in 51 blood samples [Figure - 2], all of which were also positive by PCR [Figure - 3], while 6 samples were positive for IgM antibody. Out of the 95 samples subjected to blood culture, leptospires were isolated in 27 samples. One of the isolates was a saprophyte and was obtained from a sample that was antigen negative. [Table - 1] summarizes the detection of leptospiral antigen (and culture, if any) / antibody with reference to time of collection of the blood sample after the onset of fever. It can be observed that high culture positivity was evident in samples collected in the early stages after infection. Among the 26 clinical isolates, the serovars included Australis (1), Hardjo (3), Autumnalis (1), Hebdomadis (3), Bataviae (1), Icterohaemorrhagiae (2), Canicola (1), Pomona (7), Grippotyphosa (1), Tarassovi (3), unidentified (3), thus making Pomona as the most common serovar. [Table - 2] shows the occupation and the different symptoms in these seven patients with Pomona as the causative serovar. Discussion In leptospirosis, there is poor correlation between the infecting leptospiral serovar and clinical presentations.[2] In human leptospirosis, though microscopic agglutination test (MAT) provides information about the infecting serovar, isolation and typing of the organism is mandatory for definite confirmation. In this study on 265 patients, 51 patients who were antigen and PCR positive were taken as confirmed cases of leptospirosis and 44 patients who were positive by IgM ELISA were considered as probable cases of leptospirosis as they were negative by PCR. Antigen detection in the urine in patients at one to three weeks of illness was found to be a useful diagnostic test as seen in a Thailand study.[6] In this study, we detected antigen in 26 out of 38 patients who had fever for two to four days (68.5%); PCR was also found to be positive in all these cases. When blood was analyzed at later intervals [Table - 1], the level of antigen detection was lowered. Many of these samples also proved to be positive by culture. In one sample, that was culture positive, antigen and PCR were negative. This was identified as a saprophyte by resistance to 8-azaguanine and growth at 13oC. This study thus shows that antigen detection is useful in the diagnosis of acute cases of leptospirosis. MAT was not done as all the samples were collected in the acute phase of the disease. 49 of the 51 antigen positive patients responded to treatment with penicillin, amoxycillin or doxycycline while two patients died due to severe multi-organ dysfunction syndrome at the time of admission. Acknowledgements Dr. H V Batra (DRDE, Gwalior India) is acknowledged for providing the antigen detection kits and for the help provided through out the study. References
Copyright 2006 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb06108t1.jpg] [mb06108f1.jpg] [mb06108t2.jpg] [mb06108f3.jpg] [mb06108f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}