 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
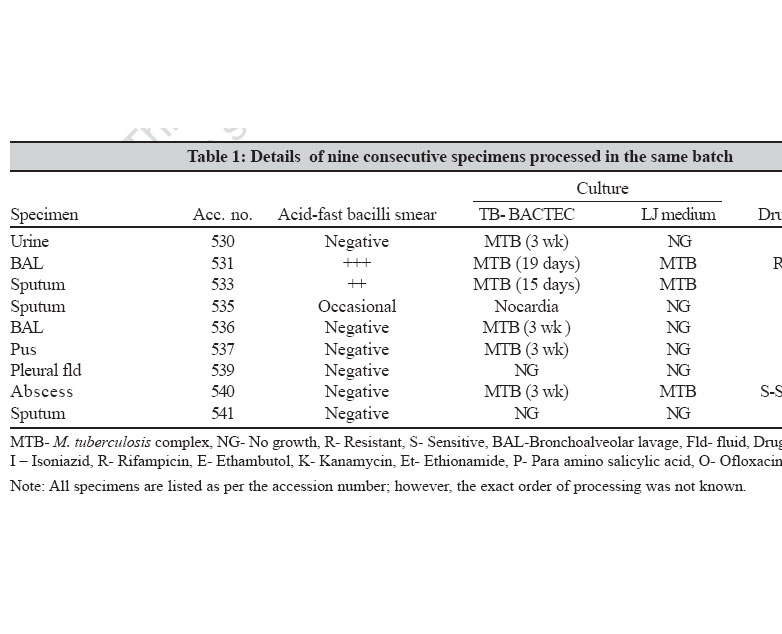
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 4-6 Special Article Dedicated decontamination: A necessity to prevent cross contamination in high throughput mycobacteriology laboratories Rodrigues C, Almeida D, Shenai S, Goyal N, Mehta A P. D. Hinduja Hospital and MRC, Veer Savarkar Marg, Mahim (West), Mumbai - 400 016, Maharashtra Date of Submission: 07-Nov-2005 Code Number: mb07003 Abstract Unrecognized cross-contamination has been known to occur in laboratories frequently, especially with sensitive recovery system like BACTEC 460 TB. In March 2001, we investigated a pseudo-outbreak of Mycobacterium tuberculosis isolates in three smear negative clinical specimens and would like to present our experience in this communication.Methods : All suspected cases were confirmed by checking the drug susceptibility and DNA fingerprints using spoligotyping as well as restriction fragment length polymorphism. Results: On investigation, the most likely cause was found to be the use of common decontamination reagents and phosphate buffer. Conclusions: To avoid erroneous diagnosis, we have devised a dedicated decontamination procedure, which includes separate aliquoting of phosphate buffer and decontamination reagents per patient. Timely molecular analysis and appropriate changes to specimen processing have been identified as useful measures for limiting laboratory cross contamination. Keywords: Cross contamination, dedicated decontamination, pseudo-outbreak Cross-contamination is an inherent problem in culturing mycobacteria.[1],[2] Unrecognized cross-contamination has been known to occur in laboratories frequently, especially with sensitive recovery system like BACTEC 460 TB system.[3] The potential impact of cross contamination results in false positive cultures which may lead to needless therapy with all its problems. Materials and Methods The mycobacteriology laboratory at PD Hinduja National Hospital and Medical Research Center, Mumbai, India, receives about 3500 requests for acid-fast bacteria cultures annually, 45% of which are positive for M. tuberculosis complex. All the specimens we receive are decontaminated by standard NALC-NaOH method[4] and then inoculated into BACTEC 12 B vial along with one Lowenstein &Jensen (L.J) slant. In this episode, suspected cross contamination cases were confirmed by antimycobacterial drug susceptibility patterns, spoligotyping and restriction fragment length polymorphism (RFLP). Drug susceptibility testing Antimycobacterial drug susceptibility of all the specimens was determined by BACTEC 460 TB system. Spoligotyping Spoligotyping was performed with a commercially available kit (Isogen Bioscience). Briefly, the procedure involved amplification of the direct repeat (DR) region of M. tuberculosis genome by polymerase chain reaction using specific biotinylated primers.[5] The amplified products were then hybridized onto a nylon membrane blotted with 43 spacer sequences. The spacer sequences were specific to the DR region and the strains differed in presence or absence of these spacer sequences. The results of hybridization were detected by ECL detection system.[6],[7] RFLP analysis RFLP analysis was performed by the internationally standardized procedure.[7] In brief, bacterial cell walls were lysed and whole genomic DNA was extracted and digested with PvuII. The resulting DNA fingerprints were separated by gel electrophoresis, transferred to nylon membrane and probed with a horseradish peroxidase-labeled 245-bp sequence of IS6110 DNA. Clinical correlation The medical records of all six patients were reviewed and the treating physicians were contacted for clinical details. The laboratory technician was interviewed to obtain information about specimen handling and processing. Confidentiality of all reports was maintained. Results A retrospective investigation was carried out after receiving the feedback of a report of M. tuberculosis complex in a patient not clinically suspected to have tuberculosis (TB). Review of laboratory records revealed that of the nine consecutive specimens processed in the same batch, six were positive by culture [Table - 1]. Of these six specimens, three were acid-fast bacilli (AFB) negative in smears, which included a urine sample, a bronchoalveolar lavage and a pus sample. All these three cultures were positive only in the BACTEC bottles almost after three weeks and yielded no growth on the accompanying LJ slants. Clinical findings for these three patients were not consistent with active TB. The drug susceptibility testing indicated multidrug resistance i.e., resistance to isoniazid and rifampicin. All the six M. tuberculosis isolates were subjected to spoligotyping. Result analysis showed the identical spoligopatterns in four out of six M. tuberculosis isolates. Review of laboratory records revealed that, of the four clinical specimens showing identical spoligotypes, one was smear positive and considered to be the index specimen. Remaining two isolates grown from smear positive specimens had different spoligotypes hence were considered true positives. Since spoligotyping is known to be less refractory for differentiation of M. tuberculosis, we also analyzed the strains using IS6110 RFLP analysis. However, only three strains (index specimen and two contaminated specimens) could be typed using RFLP due to lack of availability of adequate or good quality DNA. All these three specimens typed showed same RFLP pattern indicated by a single band. Discussion Review of literature reveals a large variation in the reported rates of cross-contamination, ranging from 0.1 to 65%.[8] Multiple factors can contribute to cross contamination, including contaminated clinical devices, clerical errors and human or technical errors that occur in the laboratory while processing clinical specimens. The last category can be caused by batch processing, laboratory protocols not adapted for left-handedness,[8],[9] sleeve of the laboratory coats of technicians touching the tubes, use of common decontamination reagents and phosphate buffer, use of a faulty exhaust hood, soiled needles or faulty needle heater circuit in the BACTEC 460 TB system.[1],[3],[8],[10] In this series, all the specimens were processed in the biological safety cabinet class II by general laboratory technician. However, the order of processing was neither according to the accession number nor in the ascending order of bacterial load. The AFB smear positive sputum samples were processed before the smear negative samples. Further investigation suggested that the cross-contamination probably resulted while dispensing decontamination reagents and neutralizing agent [phosphate buffered saline (PBS)] with a common flask. PBS was prepared in a liter quantity and the contamination might have occurred due to unintentional touching the edges of the open specimen containing tubes with the PBS flask or droplets splashed from a sample in a specimen containing tube while pouring PBS directly through the heavy flask. Since this pseudo-outbreak was recorded almost three weeks after the inoculation, the original decontamination reagents and phosphate buffer were not available for culture. Recognition of laboratory cross-contamination and elucidation of its probable cause has resulted in the revision of laboratory procedures. Instead of using general laboratory technicians, we have two full-time, thoroughly trained and experienced TB-technician dedicated to mycobacteriology. In addition two more technicians are trained for emergency back-up. To avoid cross-contamination we have devised a dedicated decontamination procedure for decontamination as given below:
In addition, we have started with a regular follow-up of all AFB culture positive patients and a timely inspection of all M. tuberculosis isolates grown in BACTEC 460 TB system by spoligotyping to validate our results. We are following these revised laboratory procedures for the past four years and the incidence of false positive cultures was not repeated again suggesting that the dedicated decontamination did play a role in eliminating the problem. Identification of cross-contaminated cultures has important consequences such as erroneous diagnosis and needless therapy. The laboratories may also be able to identify certain equipment or procedural errors leading to false positive cultures and if corrected promptly may minimize erroneous reporting. We believe that the use of dedicated decontamination is useful in minimizing cross contamination. Regular clinical feedback is vital in identifying potential cases of cross-contamination. Use of simple and rapid molecular methods aid in diagnosis of laboratory cross-contamination. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07003t1.jpg] |
| |||||||||
{kind=link}