 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
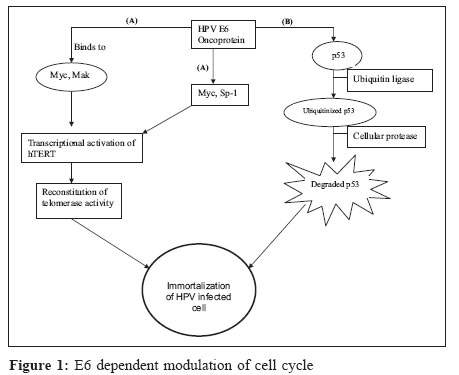
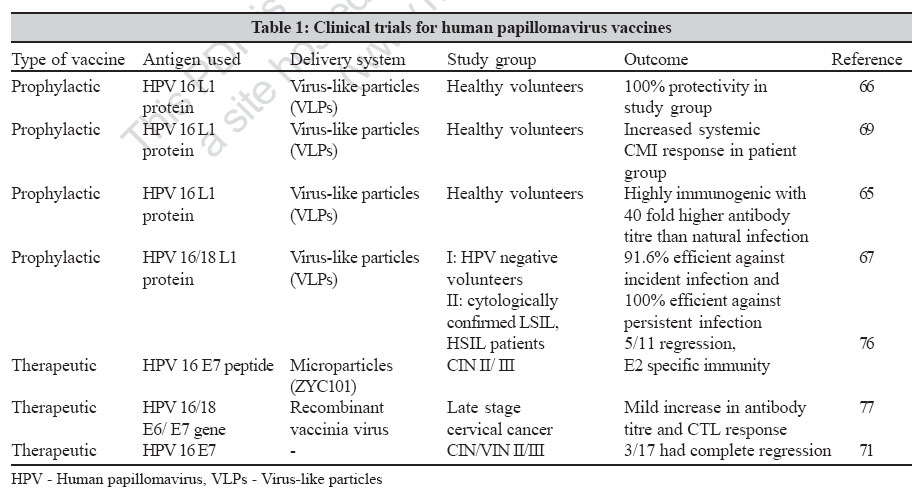
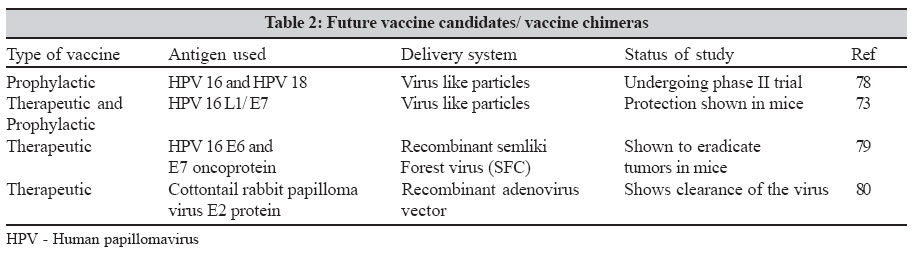
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 10-17 Review Article An overview of human papillomaviruses and current vaccine strategies Gnanamony M, Peedicayil A, Abraham P Department of Clinical Virology, Christian Medical College, Vellore - 632 004, Tamil Nadu Date of Submission: 07-Feb-2006 Code Number: mb07005 Abstract Cervical cancer is one of the most common cancers in women worldwide, particularly in developing countries. The viral origin of cervical cancer has been proven beyond any reasonable doubt. Persistent infection with certain subsets of human papillomaviruses is recognized as a necessary cause for the development of cervical cancer. Persistence of oncogenic HPVs, immunodeficiency, high HPV viral load and cofactors like smoking, multiple sex partners and poor nutrition predispose to cervical cancer. Prophylactic vaccines using HPV virus-like particles containing capsid protein L1 have shown protection against disease in animals and are currently undergoing clinical trials. Therapeutic vaccines using HPV E6 and E7 proteins are also being investigated for their ability to remove residual infection.Keywords: Cervical cancer, human papilloma virus, vaccines Epidemiological evidence has proved beyond doubt that human papillomavirus (HPV) infection is the most important risk factor for cervical intraepithelial neoplasia and invasive cervical cancer.[1],[2] HPVs infect the basal epithelium and are grouped as cutaneous and mucosal types. Based on the association with cervical cancer, genital HPVs are further grouped into high risk types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73 and 82), probable high-risk types (26, 53 and 66) and low risk types (6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81 and CP6108).[3] Of the high risk types, HPV 16 is the most prevalent type and is seen in at least 50% of invasive cervical cancer patients globally followed by types 18, 45, 31, 33, 52 and 58.[4] Various studies have looked at the prevalence of HPV genotypes in Indian women[5],[6],[7] and the most common genotypes reported are HPV 16 and 18. Basic Virology HPV are members of the family Papillomaviridae.[8] They are small, non-enveloped DNA viruses, 55 nm in diameter.[9] They have an outer icosahedral capsid made of two structural proteins, L1 and L2. The genome of HPV is circular and approximately 8 Kb long.[8] The genome has eight open reading frames coding for six early proteins (E1, E2, E4, E5, E6 and E7) and two late proteins (L1 and L2). E1 and E2 genes are involved in viral replication.[10] E2 protein also plays an important role as a repressor of E6 and E7 gene expression. E4 gene codes for protein E1-E4 that disrupt the cytoplasmic keratin network.[11] The E4 protein is also found to contribute to regulation of host cell cycle control.[12] E5 protein is known to aid in cellular transformation and plays a significant role in viral replication.[13] The late proteins L1 and L2 make up the viral capsid. E6 and E7 proteins play a major role in the malignant transformation of cervical cells as can be seen in studies using various cell lines.[14],[15] The E6 protein forms a complex with the cell cycle regulator protein p53[16] using cellular ubiquitin ligase E6AP.[17],[18] This ubiquitination was found to lead to accelerated degradation of p53.[19] The E6 protein also down regulates p53 activity by targeting the co-activator of p53, CBP/p300.[20] Inactivation of p53 leads to loss of cell cycle control such as cell cycle arrest and apoptosis. E6 protein associates with Myc/Mak proteins and Sp-1 and this complex binds to the promoter region of the catalytic subunit of telomerase enzyme, hTERT.[21],[22],[23] This leads to an increase in telomerase activity, thereby facilitating immortalization [Figure - 1]. The E7 protein associates with retinoblastoma family of proteins. The E7 protein binds to the phosphorylated retinoblastoma protein (Rb) and separates it from E2F/DP1 complex.[24] The E7 protein then mediates degradation of the Rb protein through the ubiquitin-proteosome pathway. E7 protein also binds to various other cellular proteins like cyclin dependent kinase (cdk) inhibitor p21, possibly leading to loss of cell cycle control.[25] The E7 protein also associates with another group of proteins called histone deacetylases (HDACs) independent of Rb protein and this results in the expression of E2F/DP1 inducible genes. E2F proteins activate expression of various genes necessary for cell cycle progression and DNA replication[26] [Figure - 2]. Thus the combined effect of these two viral oncoproteins and above mentioned cellular factors contribute to the malignant transformation of the cervical cells. Epidemiology Human papillomavirus is transmitted by sexual contact. However a non-sexual mode of transmission through fomites has also been proposed.[27] Epidemiological evidence also points to an association between cervical cancer and various risk factors. Impaired cell mediated immunity is a major risk factor for cervical cancer. Evidence for this is derived from studies showing a high incidence of HPV infection in human immunodeficiency virus seropositive women.[28] High HPV viral load is a risk factor associated with high stages of cervical disease.[29] Persistence of high-risk types of HPV is another major risk factor in the development of cervical cancer. A higher risk of acquiring HPV was attributed to decreasing age of first sexual intercourse, multiple sexual partners and clinical history of other venereal diseases.[30] High parity was found to increase the risk of infection.[31] Long-term use of oral contraceptives[32] is also a significant cofactor in the development of cervical cancer. Most Indian studies have reported HPV 16 and 18 as the major genotypes. There is evidence that there are other oncogenic HPV types circulating in our population. In our center, the predominant HPV types detected were HPV 16 and 18 followed by 52, 33, 58, 35, 31, 45, 51 and 56 (unpublished data). More recently, naturally occurring HPV variants are gaining importance as viral markers of epidemiology and pathogenesis. Based on sequence analysis of the E6, L1, L2 and long control region, HPV 16 is grouped into five major phylogenetic clusters. They are European (E), Asian (As), Asian-American (AA), African-1(Af1) and African-2 (Af2).[9] A study from our center has shown a higher prevelance (92%) of European (E) variant class of HPV 16 in Indian population.[33] Pathogenesis HPVs infect the basal layers of the cervical squamous epithelium through mild abrasions or trauma. HPV is thought to enter the cell after attaching to cell surface receptor heparan sulphate.[34] The virus life cycle depends on the differentiation of the host squamous epithelium. In the basal layers of the epithelium, the virus genome is episomal and establishes itself at low copy numbers. The early protein E1 in association with E2 is thought to trigger the replication process. At this stage, the expression of the viral oncoproteins E6 and E7 are kept in check by the E2 protein, which acts as a transcriptional repressor. In the terminal layers, the virus switches from theta replication to rolling circle mode of replication, resulting in a high copy number of viral DNA.[35] At this stage, the virus manages to integrate its DNA into the host chromosome. This disrupts the E2 open reading frame leading to excess synthesis of the E6 and E7 oncoproteins. This eventually is thought to lead to malignant transformation of the epithelial cells. Studies from our centre have shown that HPV 16 E6 and E7 transcripts are seen in all cases of invasive cancer but not in cases of cervical intraepithelial neoplasia (CIN) I and II. The presence of episomal E2 DNA in high propotion (52.4%) of patients with invasive carcinoma and the presence of significant variations in the E2 gene suggests that there are alternate mechanisms of E6 and E7 gene expression.[36],[37] Finally, capsid proteins L1 and L2 are synthesized and mature virions are produced. The release of HPV virions is thought to be facilitated by the E1-E4 protein. Laboratory Diagnosis The high incidence of cervical cancer in developing countries emphasizes the need for proper screening to reduce this global burden. The primary tools for diagnosis of HPV infection are cytology, histology and recently, detection of HPV DNA. Cytology and histology The Papanicolou (Pap) smear, introduced by Papanicolau and Traut in 1943, identifies changes in cells of the transformation zone of cervix caused by HPV infection.[38] Abnormal cells are vacuolated with a pyknotic nucleus surrounded by a halo and are termed as "koilocytes". The current interpretation of Pap smear is based on the Bethesda system.[39] However, cytology has its limitations. Inadequate sampling, poor sensitivity with false negative results, contaminants in the sample, have been reported.[9] Automated cytologic tests using PapNet (Neuromedical systems, Suffern, NY) and Autopap 300 QC (Neopath, Redmond, Wash) have been approved by the Food and Drug Administration, USA for screening smears to identify false negative smears. Fluid based technology also reduces false negative smear results. The specimen is collected in a preservative solution, debris is removed thereby aiding clear visualization of the cells.[40] Colposcopy and colposcopy directed biopsies are done in patients with abnormal pap smears. Visual inspection is done with the naked eye after application of 3% acetic acid solution (VIA).[9] Dysplastic cells appear as acetowhite lesions. Visual inspection with Lugol′s iodine (VILI) is another approach where the cervix is viewed with the naked eye after application of iodine solution. Normal squamous epithelial cells appear brown or almost black in colour whereas abnormal cells appear colourless, pale or mustard yellow in colour.[41] Cervical biopsy is then done to conform malignancy. Cervical biopsy is considered the gold standard for the detection of cervical neoplasia and HPV infection. HPV DNA detection HPV cannot be easily cultured in the laboratory. Therefore, molecular methods to detect HPV DNA are been used to confirm the presence to HPV in clinical specimens. The currently used techniques for HPV DNA detection are the hybrid capture second generation (HC2) assay and polymerase chain reaction (PCR). The hybrid capture assay is the only commercial kit approved by the FDA for the detection of HPV. The hybrid capture assay detects 13 high-risk types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 68) and 5 low risk types (6, 11, 42, 43, 44). Hybrid Capture 2 assay was found to be a good screening tool for the detection of cervical intraepithelial neoplasia III and invasive cervical cancer.[42] The assay works on a hybridization/ signal amplification principle and uses chemiluminescence to detect the presence of HPV.[43] Recently a prototype version of Hybrid Capture 3 has been released. The hybrid capture 3 was found to be more sensitive and equally specific like its predecessor when compared to the PCR based assays.[44] But this method does not distinguish between the different HPV genotypes. Most PCR protocols for the detection of genital HPVs use consensus primers GP5/6,[45] degenerate primers MY09/11 and its modified version PGMY09/11,[46] amplifying a wide spectrum of genital HPVs. HPV genotyping is done by nucleotide sequencing, restriction fragment length polymorphism,[47] reverse hybridization line probe assay[48] and line blot assay.[49] Quantification of HPV viral load has been done by real time PCR assays.[50] Studies including those from this centre have shown an association between the presence of HPV DNA in plasma of patients with advanced stages of invasive cervical cancer and metastasis to distinct organs.[51],[52] HPV DNA in plasma can thus be used as a marker of poor disease progression. Immunology HPV infection is transient and 70% of women clear the infection in one year suggesting the role of an effective immune system in clearing the virus.[53] Immune response to HPV is however, weak and studies using HPV virus-like particles (VLPs) have shown that antibodies are detected approximately eight months after incident HPV infection.[54] The same study also shows that women who seroconverted were 5.7 times more likely to progress to HPV associated squamous intraepithelial neoplasia (SIL) than women who did not seroconvert. These results suggest that in natural infection, antibodies to HPV are not protective and serve as a marker of disease progression. Another study showed a seroprevalence of 46% in sexually active college women infected with HPV 16.[55] The importance of cell mediated immunity in controlling HPV infection comes from studies showing increased prevalence of HPV in HIV seropositive women.[28] Cytotoxic T lymphocyte (CTL) response to HPV E6 and E7 proteins were detected more commonly in HPV 16 positive patients without CIN than in HPV 16 positive patients with (CIN), suggesting a protective role of CTL′s in HPV infection.[56] This CTL response was found to be mediated by both CD4-positive and CD8-positive T lymphocytes.[57] Lymphoproliferative responses to a HPV 16 E7 peptide 37-54 were found to be associated with regression of disease and loss of HPV infection suggesting a protective role of cell mediated immune response.[58] Treatment Treatment options for cervical neoplasia depend on the stage of the disease. Cervical non-invasive lesions are treated by ablative methods like cryotherapy, laser therapy, cold coagulation and diathermy or excisional methods like loop electrosurgical excision procedure (LEEP) and conization. In cryotherapy, abnormal tissue is frozen by an instrument and destroyed. Laser therapy uses a single laser beam to cut abnormal tissue. In loop LEEP, an electrically charged wire is used to excise the lesion. Early invasive cancers are treated with radical hysterectomy or internal/external radiation therapy. Advanced cancer patients are treated with internal/ external radiation therapy and chemotherapy.[9] Additional therapies to treat HPV infection of the cervix have also been tried. Local application of antiviral agents like cidofovir has been shown to be partly effective against CIN III lesions.[59] Various immunomodulatory agents like recombinant interferon gamma,[60] imiquinod 5%[61] have also been shown to be efficacious in CIN treatment and management. In a preliminary study, antioxidant curcumin caused a down regulation of HPV 18 transcription in Hela cell line.[62] Further studies will establish the clinical efficacy of curcumin in treatment of cervical cancer. Prevention HPV screening Screening programs have greatly reduced the incidence of cervical cancer in the developed world. Prevention programs should comprise of health education and periodic pelvic examinations, which may include direct visual inspection (DVI), VIA, VILI, pap smear and HPV DNA testing. However, large scale routine screening and treatment for cervical cancer is hard to achieve in a developing country like India. A cost-effective vaccine is therefore needed as an alternative to screening and treatment. There are two types of vaccines being developed for HPV infection, prophylactic vaccine and therapeutic vaccine. Some of the studies on vaccine trials and future candidate vaccines are summarized in [Table - 1][Table - 2]. Prophylactic vaccines prevent infection by inducing production of neutralizing antibodies. A good prophylactic vaccine should be safe and should induce long-lasting protection. Development of prophylactic vaccines for HPV is hindered by various factors. HPVs are difficult to grow in vitro . Moreover, HPVs are species specific, so vaccine evaluation in animal models is also not possible. Sub-unit vaccines using HPV VLPs, obtained by expressing capsid protein L1and L2 in both prokaryotic and eukaryotic cells are currently being used as candidate vaccines. In early animal models like rabbits[63] and canines,[64] these VLPs have shown to be highly immunogenic and also shown to elicit high titres of neutralizing antibodies. An early human trial using HPV 16 VLPs produced in insect cells showed high titres of neutralizing antibodies up to 40 times higher than in a natural infection.[65] Another randomized control trial was conducted using HPV 16 VLPs consisting of HPV 16 L1 protein expressed in yeast. This study showed complete protection from disease in the vaccinated group compared to the unvaccinated group.[66] This study has shown that HPV 16 VLPs used as prophylactic vaccines can reduce cervical cancer risk in women who are HPV 16 negative. Recently, a bivalent HPV 16/ 18 virus-like particle vaccine has been shown to be efficacious in preventing incident and persistent infections with HPV 16 and 18.[67] Quadrivalent vaccines using VLPs made of HPV 6, 11, 16, 18 have been tested for their efficacy in chimpanzees. The study shows that this vaccine elicits both neutralizing antibodies as well as a transient CTL responses.[68] Currently phase III trials are being undertaken to prove its efficacy. Another human trial demonstrated the ability of HPV VLP vaccines to induce both humoral as well as cell-mediated immune responses in healthy individuals as shown by increased neutralizing antibodies as well as cytokine response.[69] Future vaccine candidates in our country should incorporate the important prevalent high-risk HPV types. Therapeutic vaccines Therapeutic vaccines are being developed to treat already established infections. As the early oncoproteins E6 and E7 are expressed through out the lifecycle of the virus and their presence necessary to maintain the transformed state in cell lines,[70] they are potential targets as therapeutic vaccines. A phase I trial using E7 peptide vaccine showed regression of disease in the study population.[71] Vaccination with long peptides of E7 protein of HPV 16 elicited a robust CD4-positive T helper cell response as well as a CD8-positive CTL response in mice.[72] DNA vaccines comprising the HPV 16 E6 gene were shown to elicit protective cell mediated immune response in mice.[73] Chimeric VLPs have also been developed by fusing non-structural proteins E7 or E2 into L2 protein. These chimeric VLPs elicit both humoral immune responses as well as cell mediated immune responses[74] and may be relevant for a population that has established HPV related cervical disease. Conclusions HPV infection has been reported to be a frequently occurring sexually transmitted disease.[9] It has also been implicated in causing cervical cancer, which is the most frequently occurring cancer in Indian rural women. India carries a fourth of world′s burden of cervical cancer.[75] It is important that health authorities place cervical cancer screening and HPV detection as a high priority in future cancer prevention health strategies[80]. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07005f2.jpg] [mb07005t1.jpg] [mb07005t2.jpg] [mb07005f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}