 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
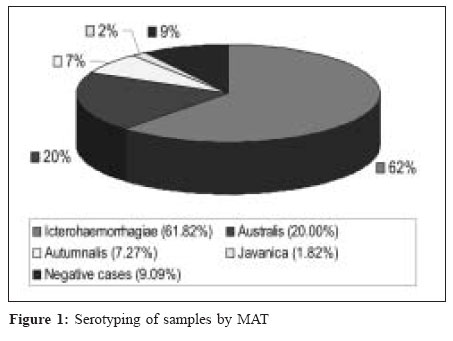
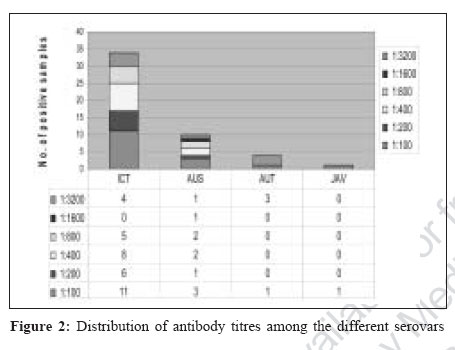
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 24-27 Original Article Serological evaluation of leptospirosis in Hyderabad, Andhra Pradesh: A retrospective hospital-based study Velineni S, Asuthkar S, Umabala P, Lakshmi V, Sritharan M Department of Animal Sciences, School of Life Sciences, University of Hyderabad, Hyderabad - 500 046 Date of Submission: 06-Feb-2006 Code Number: mb07007 Abstract Purpose : Leptospirosis is a zoonotic disease with humans getting the infection either from rodent hosts or from domestic animals. Urine contaminated environment is the common source of infection. This is an under-reported disease in Andhra Pradesh. We report a retrospective hospital-based study on 55 patients with suspected leptospirosis.Methods : A total of 55 serum samples were collected from patients with suspected leptospirosis and subjected to serological testing by LeptoTek Dri-dot, microscopic agglutination test (MAT) and IgM enzyme-linked immunosorbent assay (ELISA). Identification of the predominant infecting serotype was done using a panel of 12 serovars. Results: MAT analysis of all the 55 samples identified all cases to be positive. The predominant serogroup was Icterohaemorrhagiae (68%) followed by Australis (22%), Autumnalis (8%) and Javanica (2%). LeptoTek Dri-dot showed a sensitivity of 96% as compared to MAT. IgM ELISA done on 32 samples showed a sensitivity of 86.7% compared to MAT. Conclusions : MAT helped to identify Icterohemorrhagiae as the predominant serovar in this study. Despite the small number of samples analyzed, the data obtained establishes a need for a prospective study in this region. Keywords: Leptospirosis, leptoTek Dri-dot, microscopic agglutination test, IgM enzyme-linked immunosorbent assay Leptospirosis is a spirochetal disease caused by the pathogenic members of the genus Leptospira . It is a wide-spread zoonosis that affects humans worldwide, in both urban and rural areas and in temperate and tropical climates.[1],[2] Humans are accidental hosts and are infected by contact with an environment contaminated by urine of shedder hosts such as rodents, cattle and dogs.[3] Individuals at risk include farmers, abattoir workers, sewer workers and miners as well as all occupations related to animal holdings are at a great risk. Human leptospirosis is prevalent in several states in India, sporadically or as outbreaks, especially during rainy seasons.[4],[5],[6],[7],[8],[9],[10] Despite the morbidity and unnecessary mortality, as witnessed in the recent floods in Mumbai, there is no systematic prevention and control programme for leptospirosis in the country, as it has not been identified as priority under the national health policy.[3] With the exception of reports by Dalal[11] and Joseph and Kalra,[12] very few reports on leptospirosis originated from India till the 1980s.[7] This is in spite of the fact that the isolation of the causative organism was first reported as early as 1931, from the Andaman and Nicobar islands.[13] Seroprevalence rate of more than 55% was observed in the general population of North Andamans.[14] Studies from South India include reports of leptospirosis in several places in states of Tamil Nadu, Kerala and Karnataka.[5],[6],[10],[15],[16] In the state of Andhra Pradesh, to the best of our knowledge, there is no systematic study on human leptospirosis and the disease remains largely under-reported. In general, the two contributing factors for the gross under-reporting of leptospirosis include difficulty in clinical diagnosis due to its protean clinical manifestations and the lack of simple diagnostic measures for early detection and control of the infection. The disease symptoms range from a mild flu-like illness to a variety of clinical syndromes including hepato-renal involvement with jaundice, severe pulmonary hemorrhage, myocarditis and meningitis.[2] Direct detection of the organism from clinical material by culture and/or dark field microscopy, though providing definite proof of the diagnosis is a time-consuming procedure requiring expensive laboratory facilities and the success rate is very low.[17] Molecular methods, mainly polymerase chain reaction (PCR) assays, despite their sensitivity suffer from false positivity and cannot be used as a diagnostic test on their own and further require expensive equipment and expertise.[1] Serological tests based on the detection of antibodies remain the most practical method of diagnosis of leptospirosis. Among the serological techniques, the microscopic agglutination test (MAT) remains the "gold standard" because of its unsurpassed diagnostic (serovar/serogroup) specificity in comparison with other currently available tests. In this study, we performed MAT and IgM enzyme-linked immunosorbent assay (ELISA) on 55 serum samples obtained from patients who were clinically suspected of leptospirosis. All these samples were positive by LeptoTek Dri-Dot. Using MAT, we identified the predominant serovars among the positive cases in this hospital-based study. Materials and Methods Bacterial strains The leptospiral serovars used in this study include the following serovars in the species: a) Leptospira interrogans -Pomona (strain Pomona), Icterohemorrhagiae (strain Lai), Australis (strain Ballico), Autumnalis serovar Rachmati (strain Rachmat), Hardjo (strain Hardjoprajitno), Hebdomadis (strain Hebdomadis), b) Leptospira kirschneri serovar Grippotyphosa (strain Moskva V), c) Leptospira borgpetersenii - Tarassovi (strain Perepelicin), Javanica (strain Poi), Ballum (strain MUS127), d) Leptospira meyerii- Ranarum (strain ICF) and e) Leptospira biflexa serovar Patoc strain Patoc I. They were obtained from the Regional Medical Research Center (WHO collaborating center for diagnosis, reference, research and training in leptospirosis, ICMR) in Port Blair, Andaman and Nicobar Islands. These serovars were maintained in semisolid (0.15% Noble agar) EMJH supplemented with 10% enrichment (Difco, USA) at 30°C in screw capped test tubes. Serum samples Serum collected from patients suspected of leptospirosis were routinely tested by LeptoTek Dri-Dot (bioMerieux, The Netherlands) at the Nizam′s Institute of Medical Sciences (NIMS), Hyderabad. In this study, a total of 55 serum samples, collected during 2001-2004 were further analyzed by MAT and IgM ELISA. LeptoTek Dri-Dot test (bioMerieux, The Netherlands) Briefly, 10 μL of test serum was added and test was performed as per the manufacturer′s instructions. Aggregation of latex particles of the test dot reveals agglutination by Leptospira -specific antibodies present in serum sample. The results were interpreted as positive if fine granular agglutination settled at the edges of the blue droplet and as negative if the blue suspension remained homogenous. Strong agglutination was observed within 30 sec. Care was taken to record all the results within 30 sec. MAT The representative cultures from different serogroups were grown in liquid medium and diluted to a density equivalent to McFarland 1.0 for use in MAT. Care was taken to ensure that no culture sample with clumping or auto agglutination was used in the study. In a microtitre plate, 50 μL of serum at dilutions ranging from 1:50 to 1:3200 in phosphate buffered saline (0.1 M, pH 7.2) was added. 50 μL of specific serovar (McFarland 1.0) was added to all the serum dilutions. The antigen control included 50 μL of live antigen without addition of antibody. The plates were incubated for four hours at 37°C. A drop from each well was examined for agglutination under a dark field microscope. The endpoint titer was the highest dilution of the serum in which 50% of the leptospiral cells were agglutinated or 50% reduction in number of leptospiral cells compared to the control. Titers equal or higher than 1:100 were considered as positive.[18] IgM ELISA test (Pan-Bio, France) IgM ELISA using Leptospira biflexa serovar Patoc antigen attached to polystyrene surface of micro well test strips were performed according to manufacturer′s instructions employing 10 µl of test serum. Plates were incubated for 30 min at 37°C. HRP-conjugated anti-human IgM and the TMB in the kit were used as per instructions. Absorbance was read at 450 nm and readings were interpreted in terms of Pan-Bio units calculated as per the instructions. The absorbance of the positive control serum, negative control serum and cut-off calibrator, provided by the manufacturer was used for the calculation of Pan-Bio units. Samples were recorded as positive if the number of Pan-Bio units were more than 11. Blood Culture Of the 55 cases, blood from 20 of them was subjected to culture. Few (3-5) drops of the freshly collected blood was immediately added to 3 mL of semi-solid EMJH-enrichment medium with 5-fluorouracil (100 μM). A drop of each culture was checked by dark field microscopy from three weeks to a maximum period of seven weeks. Results This is a retrospective study of serological evaluation of 55 human subjects suspected of leptospirosis. Large number of patients (73%) came to this tertiary hospital from rural areas. All of them had fever, myalgia with chills; 52% had renal failure; 44% developed jaundice and there was one case of pulmonary hemorrhage. Most of these patients were farmers from neighbouring villages and came to the hospital several days after the initial symptoms of illness. The commercial LeptoTek Dri-Dot kit was used to test the serum from these patients. In this study, MAT and IgM ELISA were performed on these serum samples and the comparative analysis of these serological tests is presented below. Fifty of the 55 serum samples showed anti leptospiral antibodies by MAT analysis [Figure - 1] and the predominant (68%, 34/50 cases) serogroup was Icterohemorrhagiae [Figure - 1][Figure - 2]. Among the remaining cases, 11 had antibodies against Australis (22%), four against Autumnalis (8%) and one against Javanica (2%). There was no reactivity against the non-pathogenic L. biflexa serovar Patoc and L. meyeri serovar Ranarum. Serum samples with a titre of 1:100 scored as positive. [Figure - 2] represents the significant titres of antibody against the different serovars, with 16% of the positive cases showing a titre of 1:3200. Twenty of the 55 cases were subjected to blood culture but no leptospires could be detected in any of them. This may be because leptospires can be isolated and identified in the blood during early infection. Urine samples were not routinely tested by dark field microscopy in the hospital. Discussion LeptoTek Dri-Dot was done as a routine test for diagnosing leptospirosis, ensuring that the agglutination reaction was read within 30 sec, as indicated in the kit. A comparison of LeptoTek Dri-Dot with MAT [Table - 1] showed relatively high sensitivity (96%) of this test with a positive predictive value of 87%. The fact that LeptoTek Dri-Dot was able to identify 52 cases as positive can be attributed to the higher level of anti leptospiral antibodies in these patients who came for treatment late in the disease. This probably would not be the case if LeptoTek Dri-Dot was used in a prospective study for screening a population at risk, as the titres of antibodies would be low and may not be found positive in this test (as mentioned in the kit). The table shows the results of IgM ELISA performed on 32 samples. Serum samples with a value greater than 11 PanBio units were taken as positive. 28 of the 32 samples were found positive. The sensitivity as compared to MAT was found to be lower (86.7%). It would have been more appropriate to do this test on paired serum samples, as a rise in titre would unequivocally confirm the infection. This however could not be done here as paired serum samples were not available. Positive diagnosis of leptospirosis in humans is tedious and time-consuming. Performance of the gold standard MAT for routine clinical testing is expensive and requires technical expertise. Though LeptoTek Dri-dot compared favourably with MAT in this study, an evaluation of this test for routine screening of suspected cases of leptospirosis in this region has to be done. MAT analysis is essential for the effective management of the disease. Of greater importance is that MAT helps to identify the predominant serogroup in the specific geographical location. In this study, we identified Icterohemorrhagiae as the major infecting serotype, as was also seen in Mumbai[19] and Pune.[20] Grippotyphosa was implicated in Andamans[21] and Kerala.[5] In a study in Tamil Nadu, the serogroup Autumnalis was found in Chennai, Cumbum and Tirunelveli, Panama in Madurai and Icterohemorrhagiae in Bodi.[16] It is known that leptospirosis is widespread in farm and domestic animals in many parts of India including the north-east, West Bengal, Bihar, Madhya Pradesh, Maharashtra, Andhra Pradesh, Karnataka, Kerala, Tamil Nadu, Punjab and Haryana.[10] As reiterated by John,[5] fewer reports on human leptospirosis do not imply that this disease is prevalent only from these reported areas. There is a need for etiologically diagnosing leptospirosis in all hospitals as this would increase public awareness and help to deal with situations of outbreaks, as was recently witnessed in the Mumbai floods and would definitely decrease the mortality associated with this disease. In this study, we have shown that leptospirosis is prevalent in this part of Andhra Pradesh and Icterohemorrhagiae is the major infecting serotype. Acknowledgements SV acknowledges the Junior Research Fellowship given by CSIR. SA acknowledges the Senior Research Fellowship by ILS-MoU scheme of the University of Hyderabad. MS acknowledges the contribution of AP-Netherlands Biotechnology Programme and Department of Biotechnology for the establishment of containment facility and ongoing research in leptospirosis. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07007t1.jpg] [mb07007f2.jpg] [mb07007f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}