 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 28-31 Original Article Brucellosis in high risk group individuals Agasthya AS, Isloor S, Prabhudas K Project Directorate on Animal Disease Monitoring and Surveillance, ICAR, Bangalore - 560 024 Date of Submission:
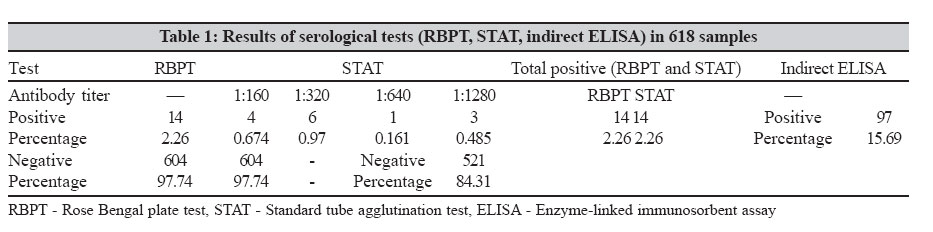
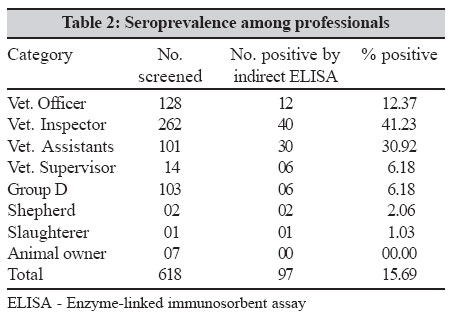
05-Aug-2006 Code Number: ph07008 Abstract Purpose: The purpose of this study was to investigate the seroprevalence of brucellosis among high-risk group individuals, consisting of veterinarians and para-veterinarians, shepherds, butchers and animal owners.Methods: The present work was carried out at Project Directorate on Animal Disease Monitoring and Surveillance, Bangalore, by using the recently developed indirect enzyme-linked immunosorbent assay (ELISA) for antibodies to Brucella abortus. Results: The results were compared with the conventional serological tests, Rose Bengal plate test and standard tube agglutination test. The result showed that the indirect ELISA was more sensitive than the conventional tests. Of 618 tested, the disease of prevalence was at 41.23% in veterinary inspectors, 30.92% in veterinary assistants, 12.37% in veterinary officers, 6.18% in veterinary supervisors, 6.18% in Group D workers, 2.06% in shepherds and 1.03% in butchers. Conclusions: This study results highlight the immediate necessity to institute control measures to control Brucellosis. Keywords: Brucellosis, professional hazard, seroprevalence, indirect enzyme-linked immunosorbent assay, zoonosis Brucellosis is one of the world′s major zoonosis that continues to be of public health and economic concern in many parts of the world. The disease is usually transmitted from infected animals to man by direct contact or by consumption of raw milk infected with Brucella organisms.[1] Brucellosis is an occupational hazard. Primarily a disease of animals, it is transmitted directly or indirectly to man. Dairy workers, shepherds, veterinarians, abattoir workers and animal husbandry personnel are particularly at risk. It constitutes an uncontrolled public health problem in many developing countries. Brucella organisms are shed in milk, urine and vaginal discharges and they thereby contaminate the environment. The infection occurs through the ingestion of unboiled milk of infected animals, contact with vaginal discharge, urine, faeces and blood of infected animals, through unbreached skin and mucous membrane of conjuctiva and also by inhalation.[2] Brucellosis is of particular concern in India because nearly 80% of Indian population resides in rural areas in close contact with livestock like cattle, sheep, goat etc.[3] The global picture of Brucellosis has shown resurgence especially in USA.[4] Brucellosis has become a major public health concern in the Saudi Arabia and the Middle East countries, as they are a traditional bedouin pastoralist society.[5] India is an agricultural country and exposure of human beings to animals is quite high. In spite of this, very limited studies on brucellosis have been undertaken in an occupationally-exposed group. Hence, the present study was conducted to assess the seroprevalence of antibodies to Brucella abortus in individuals who are in contact with animals because of their occupation. The study group involved the screening of high-risk group individuals from Tumkur, Bidar and Bagalakote districts, in Karnataka, for antibodies to Brucella abortus . Materials and Methods Blood samples were collected from 608 employees of Department of Animal husbandry and Veterinary Services from Tumkur, Bagalakote and Bidar districts of Karnataka state. Out of this, 128 were veterinary officers, 14 were veterinary supervisors, 262 were veterinary inspectors, 101 were veterinary assistants and 103 were group D workers. Two samples from shepherds, one from a butcher and seven from animal owners were also included in the group making a total of 618 samples. A detailed history of these individuals was collected which included their name, age, occupation, nature of work, history of consumption of raw milk, history of fever (nature and duration) in the past and complaints of joint pain, if any. Indirect enzyme-linked immunosorbent assay SLPS purified by hot phenol water extraction method was used as antigen. Serum from confirmed cases of brucellosis obtained from the (BLDEA Medical College, Bijapur, courtesy, Dr. B. G. Mantur) was used as strong positive serum control. The serum samples taken from healthy individuals were used as the negative serum control. The moderate positive control was prepared by diluting the strong positive serum in negative serum (1:20). Reagents were procured commercially to develop the indirect ELISA. The rabbit antihuman HRP conjugate (Bangalore Genie), O-phenylenediamine dihydrochloride (OPD), hydrogen peroxide (H 2 O 2 ), bovine gelatin (British Pharmacopocia grade 4) and 96 well ELISA plates were used. A checkerboard titration was made to establish optimal working dilutions of SLPS antigen, control sera and immunoconjugate for use in the indirect ELISA. Microtiter plates were coated with SLPS antigen of Brucella abortus 99, at 100 μL per well (10 ng) in carbonate bicarbonate buffer (PH 9.6 ± 0.05) separately and were incubated overnight at 4°C. The plates were then washed three times with washing buffer consisting of 0.002 M phosphate buffered saline (PBS). Test and control sera (1:100, 100 μL volume) were diluted in blocking buffer (1% bovine gelatin in 0.01M PBS and 0.1% Tween 20) and then added to respective wells of the plate in duplicate for test sera and in quadruplicate for control sera. Samples were incubated for one hour at 37°C and the plates were then washed as described above. The rabbit antihuman IgG HRP conjugate (1:100, 1:3000) diluted in blocking buffer was then added to all the wells and incubated for one hour at 37°C. The plates were then washed and treated with 100 μl of freshly prepared OPD solution with H 2 O 2 for 10 minutes. Finally, adding 100 μL of 1M sulphuric acid per well stopped the enzyme substrate reaction. The plates were read at 492 nm, using an ELISA micro plate reader. Interpretation of the results Percent positivity (PP) values used for acceptance of test sera data and for diagnostic interpretation were calculated as follows: Replicate OD value of test serum x 100 Median OD values of C++ control Therefore, based on the results obtained after screening large number of samples at the PD_ADMAS laboratory using the indirect ELISA, a cut off value of 33% was recommended. All samples with PP value of 33%, were retested while those above 33% were considered positive and below were considered negative. Results [Table - 1] shows the results of the serological tests in 618 samples. Analysis of the cases by the three tests showed that RBPT, STAT and ELISA detected 14 (2.26%), 14 (2.26%) and 97 (19.69%) positives respectively. Of the 97 seropositive cases, 47 were asymptomatic and rest had clinical features such as fever, joint pains, back pain etc. [Table - 2] shows
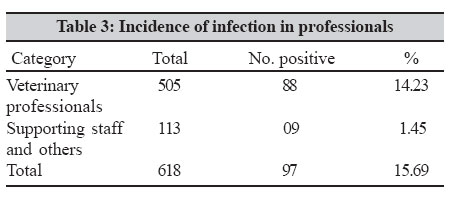
the breakup of seropositive cases by profession. None of the animal owners
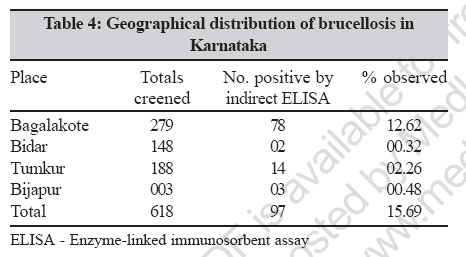
(7 samples) were seropositive. Thus the statistical analysis of the data indicated a significantly higher percentage of brucellosis recorded in veterinary professionals as compared to other supporting groups of people/shepherds. All seropositives were males except one. ( P < 0.01). [Table - 4] shows the geographical distribution of the subjects included in the study. Significant difference was found among the different areas tested for prevalence of the disease. The highest prevalence (45.36%) was found among 41-50 years age group (44 out of 97) followed by 32 out of 97 cases (32.98) in the age group of 31-40. Fourteen cases out of 97 (14.43%) were among the age group of 51-60. The least number of cases i.e. seven out of 97 cases (7.21%) were recorded in the age group of 21-30. The analysis showed a wide variation in the age group as far as the prevalence of brucellosis was concerned. Discussion Brucellosis is diagnosed either by isolation of Brucella organism in culture or by a combination of serological tests and clinical findings consistent with brucellosis. Isolation of the Brucella organism is the definitive means of diagnosis but in practice it is difficult due to the early tissue localization, exacting culture requirements of the organism and also prolonged time required for isolation. In practice blood cultures are positive in 10-30% of brucellosis and the remainder is diagnosed serologically.[2] In this study, out of 618 professionals 14 (2.26%) showed the presence of Brucella antibodies in their serum by RBPT and STAT. The titers obtained in the STAT show a high degree of correlation with those obtained by RBPT. This is in accordance with the findings of Ajay et al[7] who reported a sero prevalence of 1.14% in veterinarians. A higher rate of prevalence in veterinarians was reported by Rana et al (27.7%)[8] and Kumar et al (28.57%).[9] The classical RBPT and STAT test have shown similar results [Table - 1] in this study. RBPT test is often used as a rapid screening test. In STAT, the titers reported are in the range of 1:160 through 1:1280 IU [Table - 1]. The sensitivity of RBPT is higher than that of STAT but the specificity can be disappointingly low.[10] However, no single test provides 100% sensitivity and specificity. Keeping this in view, the analysis of all the 618 samples of the professionals showed a total of 97 positive for Brucella antibodies. The overall seroprevalence of the brucellosis was 15.69% by indirect ELISA. The indirect ELISA has the advantage of being highly sensitive, specific and economical. The ELISA used in this study can detect significantly more number of cases than RBPT and STAT. Out of 97 cases of professionals positive for brucellosis by ELISA, 16 individuals complained of intermittent fever, 10 had a history of fever, joint pain, weakness, 10 had history of chills, drenching sweat and 14 had given history of back pain and joint pain. One veterinary officer was treated for malaria was later diagnosed as brucellosis. The serum showed the presence of antibodies to SLP antigen of Brucella abortus. He had a history of undulant fever for the past six months with night sweats and sleep disturbances, chills, headache and joint pain. The blood picture revealed leukocytosis. However, nearly half the seropositives were asymptomatic. An earlier report shows asymptomatics to be 14%.[11] The seropositivity was higher in males (98.96%) compared to females (1.03%). This is different from the finding of Kapoor et al who reported higher seroprevalence in females compared to males.[12] However, in the present study, difference in seropositivity between males and females is statistically not significant which may be due to less number of female subjects in occupationally-exposed group. The present study showed that the brucellosis is still a professional hazard in the veterinary practitioners and the cases of brucellosis may be easily misdiagnosed because of the deceptive nature of the clinical signs and symptoms. All the cases that showed the presence of antibodies to Brucella abortus had varied clinical manifestations of brucellosis. The clinicians miss many cases of brucellosis because it is not considered a common disease. The clinicians should keep in mind the possibility of an occupational or environmental exposure in cases of fever. It would also be worthwhile to create awareness about the disease in such professionals so that necessary precautions and periodic screening of such occupationally exposed people can be done. Elimination of the infection in animals by vaccination to produce Brucella free animals/animal products can prevent the infection in humans. The practice of universal precautions among high-risk population cannot be overemphasized. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07008t4.jpg] [mb07008t3.jpg] [mb07008t2.jpg] [mb07008t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}