 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
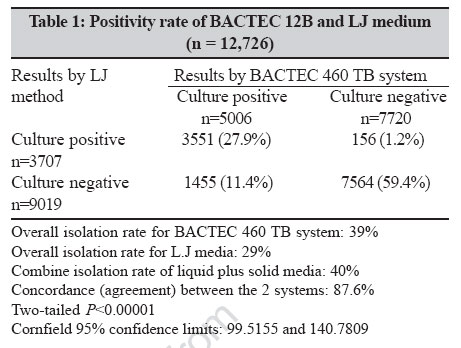
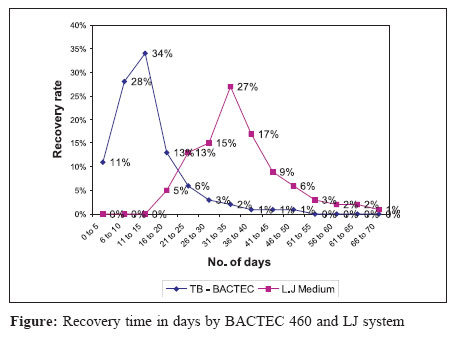
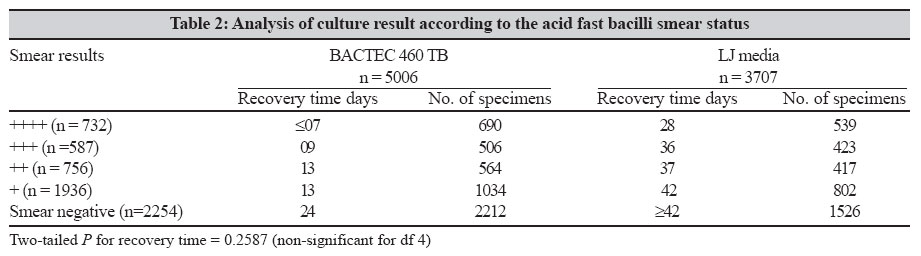
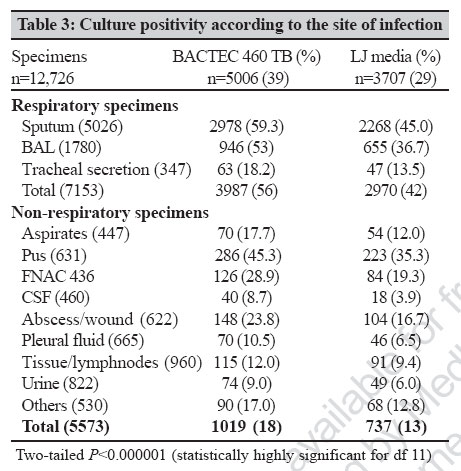
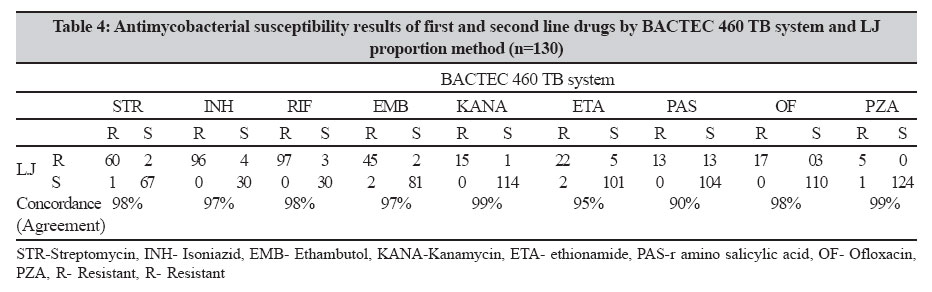
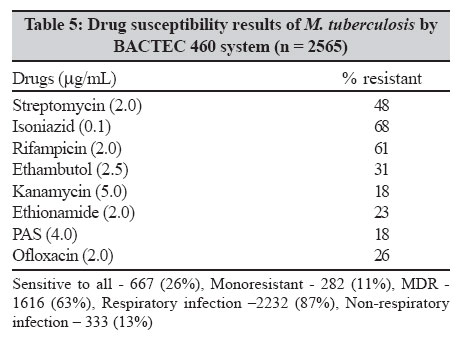
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 32-36 Original Article Use of bactec 460 TB system in the diagnosis of tuberculosis Rodrigues CS, Shenai SV, Almeida DVG, Sadani MA, Goyal N, Vadher C, Mehta AP Department of Microbiology, PD Hinduja National Hospital and Medical Research Center, Mumbai - 400 016 Date of Submission: 28-Feb-2006 Code Number: 07022 Abstract Purpose : To evaluate, the efficacy of BACTEC 460 TB system for the diagnosis of tuberculosis in a tertiary care hospital in Mumbai, India.Methods : We compared 12,726 clinical specimens using BACTEC 460 TB system and conventional method for detection of Mycobacterium tuberculosis over a period of six years. Result: The overall recovery rate was 39% by BACTEC technique and 29% using Lowenstein-Jensen (LJ) medium. An average detection time for B actec0 460 TB system was found to be 13.3 days and 15.3 days as against 31.2 days and 35.3 days by LJ method for respiratory and nonrespiratory specimens respectively. The average reporting time for drug susceptibility results ranged from 6-10 days for the BACTEC 460 TB system. Conclusions: The BACTEC system is a good system for level II laboratories, especially in the diagnosis of extrapulmonary and smear negative tuberculosis. Keywords: Acid fast bacilli culture, BACTEC 460 TB system, Mycobacterium tuberculosis Acid fast bacilli (AFB) culture is usually considered a gold standard for the laboratory diagnosis of tuberculosis (TB). Most of the mycobacteriology laboratories in India continue to depend on conventional Lowenstein and Jensen (LJ) media for culture, however, the time required and frequent negative results with paucibacillary specimens are important limitations. It is well known that the use of liquid based culture system improves the recovery with shortening of the time required to detect TB. Among the methods utilizing liquid media, semi-automated radiometric BACTEC 460 TB system (Becton Dickinson, Sparks, MD, USA) is the most widely accepted as the reference standard in the developed nations. The detection of mycobacterial growth in BACTEC 12B medium is carried out by quantitatively measuring of the 14 CO 2, liberated by the metabolism of 14 C-labelled substrate present in the medium. The system gives results of culture and Antimycobacterial Drug Susceptibility Test (AST) within 10-14 days. However, there are only about 37 installations of BACTEC 460 TB system in India, suggesting it has not been used frequently in our country. BACTEC 460 TB system was launched at our institute in 1998 and we have processed a large number of specimens since then. More recently a non-radiometric BACTEC MGIT 960 TB system has been introduced, which is better automated with no issues of radioactive disposal. As this new non-radiometric system is going to replace the radiometric TB system, we felt the need to analyze our data with BACTEC 460 TB liquid system to evaluate its performance and its contribution to our TB diagnosis before adopting another liquid culture system. Materials and Methods The data has been analyzed for six years from December 1998 to June 2004. All the clinical specimens received were subjected to direct smear microscopy by Ziehl-Neelsen (ZN) staining method. Specimens, which contain normal bacterial flora, were decontaminated by standard N-acetyl-L-cysteine-NaOH method.[1] Specimens from sterile sites were centrifuged and the sediment was inoculated into the BACTEC 12 B vial supplemented with the antimicrobial mixture PANTA (Becton Dickinson, Sparks, MD, USA). One LJ slant was also inoculated. All the inoculated media were incubated at 37 ± 1°C. Inoculated LJ slants were incubated for 8-10 weeks and checked everyday for growth for the first week after which they were inspected weekly for 10 weeks. All inoculated 12 B vials were tested twice a week for first three weeks and then once a week for remaining three weeks. Positive vials were subjected to smear microscopy. Final identification of M. tuberculosis complex (MTB) was done by the BACTEC NAP (r-nitro-α-acetylamino-β -hydroxy propiophenone) differentiation test (Becton Dickinson, Sparks, MD, USA). Obvious turbidity or sudden increase in growth index (GI) to high levels indicated contamination. This was confirmed by Gram staining of smear as well as subculture on blood agar medium. In addition, 0.2 mL of positive BACTEC broth was subcultured onto one more LJ slant. Growth on this LJ subculture was used to rule out mixed infection, for biochemical identification of MTB and non tuberculous mycobacteria (NTM) strains. Quality control of the instrument Performance test was run daily according to the manufacturer′s instructions. Maintenance of the needle heater, filters, media trap and UV light was strictly followed to prevent cross-contamination. Needles were changed daily. Quality control of the 12 B growth medium and NAP disk was carried out using standard H 37 Rv strain of M. tuberculosis . Antimicrobial susceptibility Test (AST) by BACTEC 460 TB system AST for four primary first line and four second line anti-TB drugs was performed only on request, using BACTEC 460 TB system. The first line drugs were provided in a drug kit (Becton and Dickinson) and second line drugs were acquired from local pharmaceuticals. Following concentrations were used-Streptomycin (STR) 2.0 mg/mL, isoniazid (INH) 0.1 mg/mL, rifampicin (RIF) 2.0 mg/mL, ethambutol 2.5 mg/mL, kanamycin (K) 5.0 mg/mL, ethionamide (ETA) 5.0 mg/mL, r amino salicylic acid (PAS) 4.0 mg/mL and ofloxacin (OF) 2.0 mg/mL. Drug susceptibility testing was done using standard procedure. Briefly, O.1 mL of the appropriate drug solution was injected into labeled 12 B vials which resulted into the desired concentration of a drug in the medium. This was followed by inoculation of 0.1 mL of bacterial suspension from a positive 12B vial with a GI 500-800. For control, the bacterial inoculum was diluted 1:100 before inoculation. The inoculated 12B vials were incubated and read daily on the instrument till the GI of the control reached> 30. When growth from a solid medium was used, a well-dispersed suspension (approximately corresponding to McFarland no. 1 standard turbidity) was prepared from a fresh culture. These suspensions were used in the same manner as a BACTEC positive vial described above. Reference strain of M. tuberculosis H 37 Rv was used as a batch quality control on a weekly basis. Results Of the total 12,726 clinical specimens from 9226 patients, 79% (7288) were received from out door (OPD) patients and 1938 (21%) from hospital admitted patients. Further analysis of all the OPD clinical specimens, revealed that 41% were consulted by our hospital physicians. Another 30% were referred to us by general practitioners or family physicians, 14% from private hospitals / nursing homes and 12% from government hospitals. In about 3% of cases the exact information was not available. Of the 12,726 clinical specimens 7153 (56.2%) were respiratory specimens and 5573 (43.8%) non-respiratory specimens. Overall, M. tuberculosis was isolated in 5162 specimens whereas NTM were isolated in 380 specimens by both the culture methods. The overall recovery rate was 39% for BACTEC 12B and 29% for LJ medium [Table - 1]. Compared to the conventional LJ method, BACTEC 460 TB system detected a total of 1455 (11.4%) additional positive cultures, which is statistically highly significant. Of the 156 BACTEC negative LJ positive cases, 112 were clearly negative by BACTEC whereas in 44 cases NTM was isolated by BACTEC and M. tuberculosis was isolated by LJ. A mixed growth of M. tuberculosis and NTM was identified in two cases showing two different types of colonies on LJ slant. A combination of liquid plus solid media showed a higher recovery rate of 40% [Figure - 1]. As shown in the figure, majority of the clinical specimens (73%) were positive by BACTEC during first two weeks of incubation however, LJ took a longer time. Most of the specimens were positive by LJ between four to eight weeks. An average detection time for TB-B actec0 was found to be 13.3 days (excluding the time required for Nap differentiation) compared to 31.2 days by LJ method (excluding the time required for species identification) in case of respiratory specimens. However, in case of nonrespiratory specimens an average detection time was found to be 15.3 days for TB-BACTEC compared to 35.3 days by LJ method. [Table - 2] shows the analysis of recovery time and recovery rate according to the smear positivity. Smear-negative cases were picked up in about 24 days by TB-BACTEC which compares to the time taken by LJ in 4+ smear positive cases. Of the total 2254 smear negative culture positive cases by any medium, 2212 were positive by BACTEC (98%) whereas only 1526 (68%) were positive by LJ. In [Table - 3] culture positive data was analyzed according to the site of infection from where the clinical specimens were collected. BACTEC was found to be more sensitive (statistically significant) in detecting more number of MTB from respiratory as well as non-respiratory specimens especially in cases of cerebrospinal fluid (CSF) and pleural fluids. AST of first and second line drugs by BACTEC 460 TB system and LJ proportion method has been shown in [Table - 4]. Of the total 130 culture isolates tested 100 were multi-drug resistant (resistant to atleast rifampicin and INH with or without resistance to other antimycobaterial drugs) and 30 were pansusceptibile (sensitive to all the drugs). Drug susceptibility results of 2565 cultures using BACTEC 460 TB system are summarised in [Table - 5]. Discussion The efficacy of the BACTEC 460 TB system in the detection of mycobacteria from clinical specimens has been demonstrated in a number of field trials and clinical correlation studies.[2],[3],[4],[5] Analysis of our data revealed that BACTEC 460 TB system is significantly superior than LJ medium in our settings for rapid isolation and identification of MTB from respiratory as well as non-respiratory specimens. With a total of 5162 positive cultures by any medium, 97% were positive by BACTEC with 28% positive in BACTEC only. On the other hand, 72% of the total cultures positive were positive by LJ with only 3% were positive on LJ only. Looking at the overall recovery from specimens, a statistically highly significant difference ( P < 0.00001) in recovery rate was demonstrated by BACTEC 460 TB system. The performance of BACTEC 460 was more prominent in smear-negative specimens. Of the 2254 smear negative culture positive specimens MTB was correctly isolated in 98% of the specimens compared to only 68% by LJ. The system was found to be more advantageous, in paucibacillary specimens, especially in case of extra-pulmonary cases like CSF, body fluids and fine needle aspiration cytology, where LJ media yielded very scanty growth or no growth. A more careful analysis was done on those specimens, which were positive by LJ and negative by BACTEC. Of the 156 only L.J positive MTB cases, BACTEC yielded no growth in 112 cases while NTM were isolated in the remaining 44 cases instead of MTB. Most of the BACTEC negative LJ positive strains were isolated from pus, abscesses or tissue biopsies indicating; some strains of mycobacteria require high protein egg-based media to grow. Of the 44 NTM positive in BACTEC, mixed growth (two different types of colonies on LJ) was observed in two cases, however, in 42 cases NTM (mostly rapid growers) were possibly contaminants. There was a possibility that growth of NTM in BACTEC had masked the growth of MTB. Being a liquid medium, colonized mycobacterial flora or other mycobacterial contaminants especially rapid growers, were also detected by the system. Hence reports showing NTM infections should be clinically correlated or confirmed by testing more number of specimens (at least 3).[6] Apart from NTM, bacterial or fungal contamination rates for BACTEC 460 TB system and LJ were found to be 3% and 8% respectively. Being an egg-based medium, LJ is more prone to the fungal contamination resulting in total loss of the medium. The advantage of BACTEC 12 B medium over LJ is that if it gets contaminated, the medium can be processed again for decontamination to recover mycobacteria. The major advantage of the BACTEC 460 TB system is the early availability of results. It was observed that as many as 73% yielded a positive result by BACTEC within 15 days as against none by the conventional method. It was also observed that with heavy smear positives (4+,3+) growth was seen in < 5 days compared to 24 days in smear negative specimens. Contrast to the other studies,[7] the mean recovery time required to isolate MTB, for TB-BACTEC and LJ was slightly higher in our lab. This could be attributed to the type of patient population included. Being a tertiary referral center, most of the clinical specimens we received were from the patients receiving the anti-TB treatment. We do not have complete data on the treatment status of the patients but on an average about 53% patients were receiving anti-TB treatment, which could increase the recovery time. Once a presumptive diagnosis of tuberculosis is established, an early result on drug susceptibility is vital for effective treatment of the patient, particularly when resistance to one or more drugs is suspected. The LJ medium requires four weeks for the AST results to become available. There are other concerns in using LJ medium for AST. Since LJ drug medium is made in the laboratory, there is less standrdisation and quality control in prepation of the drug medium. It is also possible that inspissation of LJ medium, binding of the drugs to proteins and storage of the prepared medium and prolonged incubation period could result in loss of potency of the drugs.[8] Further, in the conventional methods, lack of standardisation in methodology and definitions of resistance used may cause errors in the interpretation and validity of the results. Susceptibility testing of MTB by BACTEC 460 TB system is based on the modified proportion method and is FDA approved for first line anti-TB drugs. The medium and the procedure is standardized to increase the accuracy of the results. Initially, we compared susceptibility results with LJ proportion method in 130 clinical isolates (unpublished data).[9] The concordance ranged from 97 to 98% for first line drugs and 90 to 99% for second line drugs [Table - 4] . We continued with BACTEC 460 TB system, as there is no gold standard, especially in case of second line drugs. Another advantage is that the susceptibility results are available within 6-10 days compared to two to four weeks by LJ. This means that we could report complete results of isolation, identification and AST of the isolated culture within an average of 4 weeks time, a CDC recommendation.[10] The early availability of AST results would be especially beneficial to patients harboring multidrug resistant organisms to enable them to receive effective treatment with appropriate regimens. At our institute multidrug resistance (MDR) TB was found to be as high as 65%, which could be attributed to the fact that ours is a tertiary referral center and most of the patients are more likely to have been unresponsive to therapy or had relapse resulting in a bias toward drug resistant isolates.[11] In institutions dealing with referral cases with high prevalence of drug resistance, availability of a liquid media system is extremely important. Certain concerns associated with the BACTEC 460 TB system include the need for syringe and needle for inoculation, use of radio labeled products and its disposal and finally the cost. BACTEC 460 TB system involves high initial investment of 20 lakhs rupees and the high cost of culture medium. Technical support for repairs and maintenance is adequate and cost-effective. In India, an average cost for isolation and identification using BACTEC 460 TB systems is Rs. 475 per patient as compared to Rs. 40 using LJ medium. Similarly the cost for AST to SIRE using BACTEC 460 TB system is Rs. 1000 vs Rs. 250 using LJ. Thus, in developing countries, such as India, LJ is cost-effective, however, a careful analysis needs to be done to look at time to report results and its cost benefit in the long run. It takes four to six weeks for primary isolation of TB bacilli using LJ. Once isolated, species identification or drug susceptibility testing can take another four to eight weeks and during subculturing the isolate could be lost or get contaminated. Even if, biochemical tests for identification are inexpensive they are time-consuming and many times give ambiguous results. In contrast, BACTEC 460 TB system, though expensive, offers certain advantages like speed, higher recovery rate and accurate drug susceptibility testing. Moreover, cost of the BACTEC 460 TB system could be partially offset by the ease of use and early availability of reliable results. It could be extremely crucial in a region with high prevalence rates of TB, particularly in the non-respiratory and paucibacillary smear negative forms of TB. Automated MGIT is a newer version state-of-the-art machine, which would eliminate the concern of handling radioactivity and needles. However, one has to evaluate this newer system as the identification of isolated mycobacteria is not fully standardized like NAP on BACTEC. The alternative option of molecular based techniques (probe hybridization) may be expensive in routine laboratories. Acknowledgement We would like to thank Dr. Salman Siddiqui for all his help and guidance. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07009t5.jpg] [mb07009t3.jpg] [mb07009t4.jpg] [mb07009t2.jpg] [mb07009f1.jpg] [mb07009t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}