 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
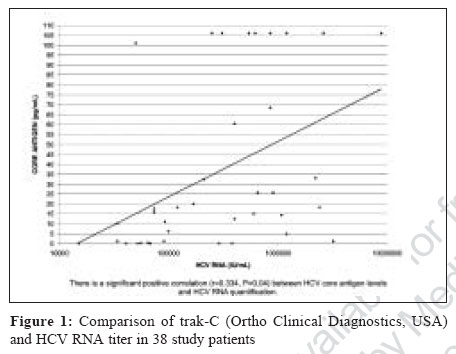
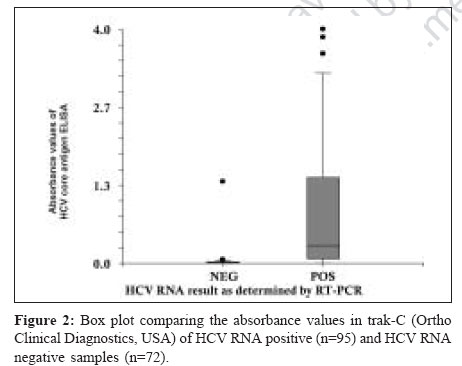
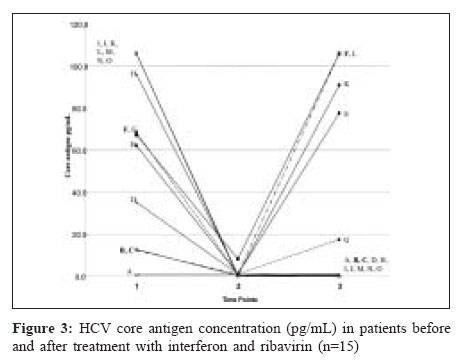
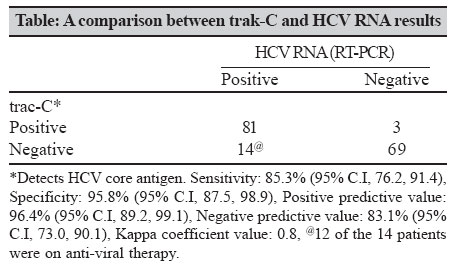
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 37-42 Original Article Significance of the hepatitis C virus (HCV) core antigen as an alternative plasma marker of active HCV infection Daniel HDJ, Vivekanandan P, Raghuraman S, Sridharan G, Chandy GM, Abraham P Department of Clinical Virology, Christian Medical College, Vellore - 632 004, Tamil Nadu Date of Submission: 07-Feb-2006 Code Number: mb07010 Abstract Purpose: To evaluate the role of core antigen (Ortho trak-C assay) as a marker of active HCV infection in comparison to HCV RNA as detected by reverse transcription polymerase chain reaction (RT-PCR).Methods: This evaluation was carried out during January 2000 to December 2003 in HCV infected individuals who were treatment naοve or were on anti-viral therapy. Additionally, sequential plasma samples from patients on clinical follow-up were included in this study. A total of 167 samples from 61 patients were tested by trak-C and RT-PCR. HCV RNA detection was achieved by a RT-PCR. Trak-C assay results were also compared in a limited proportion of these samples with known HCV viral load and genotype. Results: Of 167 samples tested, 56.9% were RNA positive and 43.1% were RNA negative while 50.3% were trak-C positive and 49.7% were trak-C negative, yielding a sensitivity of 85.3% and a specificity of 95.8% for the trak-C assay (Kappa co-efficient = 0.8). The concentration of HCVcAg and HCV RNA showed significant correlation (n=38, r=0.334, P =0.04). The trak-C assay detected the most prevalent HCV genotypes in India without significant difference ( P =0.335). The difference between mean absorbance values of HCV RNA positive samples compared to HCV RNA negative samples in the trak-C assay was highly significant ( P <0.000). Qualitative results of trak-C assay and RT-PCR were comparable in 93% of follow-up samples. Conclusions: Trak-C assay can be recommended for confirmation of HCV infection and follow-up in laboratories with resource-poor facilities. Keywords: Anti-viral therapy, hepatitis C virus core antigen, reverse transcription polymerase chain reaction, trak-C Hepatitis C virus (HCV) is a parenterally transmitted hepatitis virus infecting approximately 3% of the world population. About 20 million people in India alone are infected as estimated by a reported HCV antibody (HCV-Ab) prevalence of 1.8%.[1] Screening of blood donations, achieved mainly by serological identification of HCV-Ab, has largely reduced transmission of HCV.[2] However, antibody detection is not a reliable marker in the pre-seroconversion phase of infection, for monitoring individuals on anti-viral therapy or for assessing stage of infection. Additionally HCV-Ab is not a useful marker for individuals on immunosuppressive therapy or in those with impaired immunity. To overcome these shortfalls of antibody screening for HCV, a sensitive and specific assay such as reverse transcription polymerase chain reaction (RT-PCR) to detect HCV RNA has been the recommendation till-date. This procedure however requires technical expertise, dedicated laboratory space, is time consuming even with automation and is expensive. Therefore, there is a need to develop newer assays, which are cost-effective, sensitive and easy to perform and can reduce the serological window period to identify HCV viraemia. The HCV core antigen testing to screen individuals, who were negative for HCV-Ab[1] was first described in 1996.[3] This was further improved in 1999 with the addition of an immune-complex dissociation step, allowing the identification of core antigen in the presence or absence of HCV-Ab.[4] Recent reports suggest that the improved assay with the immune-complex dissociation step can be used for diagnosis of acute HCV infection,[5] for assessing chronic infection with HCV[6] and to monitor response to anti-viral therapy.[7] In this study we have evaluated a new commercially available enzyme-linked immunosorbent assay (trak-C Ortho Clinical Diagnostics, Inc. Raritan, New Jersey) for the detection and quantitation of HCV core antigen (HCVcAg) in plasma/serum samples in the presence/absence of HCV-Ab. It was also attempted to determine the utility of this assay for assessing virological response in patients on anti-viral therapy. Materials and Methods Clinical samples One hundred and sixty seven samples were included from 61 patients whose sequential samples were available in the clinical virology laboratory at the Christian Medical College, Vellore. As part of clinical investigations these samples were sent to the laboratory for HCV RNA detection, during the period January 2000 to December 2003. The patients were referred from the Gastroenterology and Nephrology units of this tertiary care center, comprising treatment naοve individuals and those on anti-viral therapy. Among this study group, fifteen patients had provided samples before, after and while on anti-viral therapy. Blood samples were collected after verbal consent in EDTA containing tubes and separated plasma was stored in aliquots at -60°C. HCV-Ab screening, RT-PCR and trak-C assays were done on separate aliquots of the same sample. Antibody confirmation and RNA quantitation was done on samples for which additional aliquots were available. Antibody screening and confirmation Detection of HCV-Ab was done using a third generation enzyme-linked immunosorbent assay (ELISA) (UBI HCV EIA 4.0, United Biomedical Inc. USA) and/or by AXSYM (HCV version 3.0, Abbott Laboratories, Illinois). Results were calculated based on the cut-off absorbance value calculated for each ELISA run. All samples above the cut-off absorbance value were considered positive by ELISA. The signal: cut-off ratio (S/CO) was automatically calculated by the AXSYM. Samples with S/CO values> 1.0 were considered positive by AXSYM as per the manufacturer′s instruction. In order to assess the role of HCV-Ab in influencing trak-C results, all samples, which were RNA positive and trak-C negative were tested using recombinant immunoblot assay (RIBA-HCV 3.0 SIA Ortho Clinical Diagnostics, Inc. Raritan, New Jersey). The assay was carried out and interpreted as per manufacturer′s instruction. HCV RNA detection A qualitative nucleic acid testing was performed on all the samples. RNA was obtained using the Qiagen extraction protocol (QIAamp Viral RNA Mini kit, Qiagen, Germany) and a sensitive in-house nested RT-PCR standardized in this laboratory[8] using primers specific for the 5´ noncoding region of the HCV genome was employed.[9] On samples (n=38) that had additional aliquots, HCV RNA quantitation was done using a commercial assay (Amplicor HCV MONITOR version 2.0, Roche Diagnostics, New Jersey, USA). Genotyping was done on 22(36%) samples by a type specific PCR method as standardized in this laboratory.[10] HCV core antigen assay Plasma samples were tested for the total core antigen using the trak-C assay according to the manufacturer′s instruction. The sample was treated with 100 μL of pretreatment buffer and kept in a 56°C water bath for complete dissociation of the HCV core antigen-antibody complex. Hundred microlitres of the pre-treated sample and control samples were mixed with 100 μL of the reaction buffer and incubated at room temperature (RT) in the wells coated with HCVcAg specific monoclonal antibody with agitation. The plates were washed and incubated for 30 minutes at RT with 200 μL of conjugate. Plates were washed again and incubated at RT with 200 μL of substrate. After the addition of 50 μL of stop solution the optical density of the samples, controls and the standards were read in an ELISA reader (μ-quant, Bio-Tek instruments, USA) at 490 nm using 620 nm as the reference wavelength. The concentration of core antigen was calculated in pg/mL by a standard graph with the absorbance values of the standards provided by the manufacturer. The concentration of standards ranging from 0 pg/mL to 100 pg/mL. All the samples were tested in singleton and results interpreted following the manufacturer′s instructions, samples were considered positive when the concentration of total core antigen was ≥ 1.5 pg/mL Statistical analysis Statistical analysis was performed using the statistical packages Epi info (version 6.04b) or the NCSS/PASS 2000 Dawson edition or the Microsoft Excel 2002 (Microsoft Office XP) for statistical computations where appropriate. Results were considered statistically significant at P < 0.05. Results Of the total number of 167 samples tested, 95 samples were positive and 72 were negative for RNA. Of the 95 RNA positive samples tested 81 (85.3%) were positive in trak-C and 14 (14.7%) samples were negative by trak-C. Of the 72 samples that were negative for RNA, 69 (95.8%) were negative and 3 (4.2%) were positive by trak-C. Accuracy indices of the trak-C assay are shown in the Table. The degree of agreement shown between RT-PCR and core antigen for HCV detection as indicated by the kappa coefficient was 0.8. Of the 61 patients studied, 49 were RNA positive and 12 were RNA negative. In 34 of the 49 patients who were initially RNA positive, RNA status varied in the sequential samples drawn from these patients, while 15 patients were consistently RNA positive. Eight of the 12 RNA negative patients were also negative for HCV-Ab. Eleven of the 14 RNA positive, trak-C negative samples were tested using RIBA. Seven out of eleven were positive for all the antigens. Three out of the remaining four samples were positive for c100(p), 5-1-1(p), c33c c22(p). The remaining samples were positive for all the antigens but showed a band against human superoxide dismutase (hSOD) and were hence deemed indeterminate. A total of 38 samples were quantitated for HCV RNA in IU/mL and compared with HCVcAg levels in pg/mL as shown in a scatter plot in [Figure - 1]. HCV genotype of the 22 (36%) patients was as follows: genotype 3 (n=13), followed by genotype 1 (n=7) and genotype 4 (n=2), these 22 patients were trak-C positive. The trak-C assay detected the most prevalent Indian genotypes without significant difference ( P =0.335). The mean absorbance value of HCV RNA positive samples in trak-C assay was significantly higher than the mean absorbance value of HCV RNA negative samples ( P < 0.000) [Figure - 2]. The core antigen levels of the fifteen patients (A-O) for whom samples were available before, after and during anti-viral therapy are shown in [Figure - 3]. Core antigen levels dropped while on therapy and increased after therapy for non-responders. We have tried to correlate core antigen levels on a group of patients (n=15) on anti-viral therapy [Figure - 3]. These 15 patients had given blood samples at three different time points: before, after and while on anti-viral therapy. HCVcAg titers and HCV RNA (not shown) are compared in [Figure - 3]. Of these 15 patients, three patients (patient No. F, B and C) showed discordance between HCVcAg and HCV RNA results at one of the three time points. Patient number ′F′ was positive for HCVcAg while on therapy while HCV RNA was negative. However, after therapy both HCVcAg and HCV RNA were positive suggesting that this patient is a non-responder. Of the two remaining samples, patient no. B was HCV RNA positive after therapy while HCVcAg was negative, while the other patient no. C was negative for HCVcAg while on therapy while HCV RNA was positive. However, the subsequent sample (after therapy) from patient C was negative for HCVcAg and HCV RNA. Discussion HCV RNA is the gold standard for detection of HCV infection. New molecular techniques to detect and quantify HCV RNA are available and many studies have tried to establish a relationship between viral load, disease severity and progression of the disease. Further, in order to reduce the residual risk of HCV transmission through blood banks it was made mandatory for European Blood banks in January 2, 2002 to test every blood and plasma donation for either HCVcAg or HCV RNA.[11] In previously reported studies, HCVcAg was detected one day later than HCV RNA in patients undergoing seroconversion but the sensitivity of this assay did not match the sensitivity shown by a single donor nucleic acid testing (NAT) in detecting early HCV infection.[12],[13] However, HCV RNA detection for single donations is not a feasible option because of the exorbitant cost, infrastructure and requirement of specially trained personnel. But many developed countries have introduced NAT in their blood banks using the pool testing method to reduce costs. However, pooling of samples reduces the sensitivity of the assay compared to single donor NAT. Hence core antigen is considered an alternative to NAT because single donations can be tested; it is less expensive and does not require specific infrastructure and trained personnel. Trak-C is an improvement on the core antigen assay because it is suitable to test antibody positive and antibody negative samples. The superior sensitivity of the trak-C may be attributed to the dissociation step and the new conjugate used in this assay. Our study demonstrates that HCV RNA status correlates with the HCV core protein profile in chronically infected individuals (Kappa = 0.8). The significantly higher absorbance values of trak-C in RNA positive samples corroborate this observation [Figure - 2]. The assay exhibited a sensitivity of 85.3% and a specificity of 95.8% as compared to HCV RNA detection, which is lower, compared to earlier studies, which show 100% specificity.[14],[15] This may be due to heterogeneity of the study patients with regard to risk factors and treatment status. Of the 61 patients in this study with sequential samples, 45 (74%) patients showed consistent results as compared to HCV RNA result and 16 patients showed discordant results compared to HCV RNA. Of these 16 patients, 15 were on anti-viral therapy, suggesting that the discrepancy could be due to anti-viral therapy. Fifteen of these sixteen patients were however concordant for at least one of the sequential sample drawn from these patient. One patient was consistently negative by trak-C for all follow-up samples while RNA was positive. There have been a few studies, which have tried to correlate core antigen levels with HCV viral loads. Bouvier-Alias et al reported that one pg/mL is approximately equal to 8,000 IU/mL.[16] Other studies including those involving chronically infected individuals have reported that the lower limit of detection of trak-C corresponds to viral RNA titers of 10 4 IU/mL.[17],[18] In the present study, we have attempted to evaluate the relationship between HCVcAg concentration and HCV RNA loads. A total of 38 samples from this study panel were compared. The HCV core antigen concentration correlated significantly with HCV RNA titer (r=0.334, P =0.04). However, it is known that the correlation between HCV RNA and core antigen levels may vary between patients.[19] The observation of high virus load (10 6) and low core antigen levels in five patients [Figure - 1] may be the result of ongoing anti-viral therapy in these patients. Quantitation was performed on 11 of the 14 HCV RNA positive samples, which were negative by trak-C. Eight out of fourteen samples were below 10 4 IU/mL, two samples were 10 5 IU/mL and one was 10 6 IU/mL of plasma. Our data therefore suggests that the lower detection limit of core antigen is approximately 10 4 IU/mL, which is in agreement with earlier published studies. It is noteworthy that 12 of these 14 samples missed by trak-C [Table - 1] were from patients on anti-viral therapy. Of the 14 samples deemed negative by trak-C [Table - 1] RIBA results were available for 11 samples. All the samples showed 4+ reactivity to the core antigen and other antigens as well. It is possible that this robust antibody response in these patients contributed to the lack of dissociation of antigen-antibody complexes in the pre-treatment step thereby leading to false negative results. Alternatively it may be speculated that incomplete HCV viral core particles, may lack the necessary antigenic site needed for binding with monoclonal antibody that is coated on the wells of the trak-C assay hence rendering them negative in this assay. It is known that even in other viral infections such as that with hepatitis B virus, nucleic acid concentration as determined by PCR does not correlate with the viral antigen concentration in the peripheral blood circulation.[20] Forty-two out of 45 (93.0%) samples, from patient on follow-up, showed good correlation on qualitative results of HCVcAg and HCV RNA tests. Hence our study using the trak-C assay on a limited population of patients on anti-viral therapy seems to predict response in a manner similar to other studies.[18] Trak-C is a simple and reliable direct method for detection of HCV infection. Since this assay is based on ELISA technology, it can be easily performed in most laboratories and is cost-effective. Further it does not need any specially trained personnel, special equipment or infrastructure except that which is required for ELISA tests. It also reduces the problems of possible cross contamination and false positives as in a nested PCR protocol. Hence it is a suitable alternative to HCV RNA detection. HCVcAg is also more stable as compared to RNA, the latter more likely to be degraded by the RNAase in the blood sample. It would also serve as a good direct HCV detection method in patients who are immunosuppressed. Further this assay could be employed during pre-seroconversion period when the antibody assays are negative. During the pre-seroconversion period the viral load is in the range of 10 6 to 10 8 IU/mL wherein the trak-C could be expected to be positive. However, there are individuals who during their pre-seroconversion period may have low viral load (< 10 4) which will not be detected by this assay.[17],[18] The core antigen assay may thus require further fine tuning prior to its use as a screening assay in blood banks. The Indian population harbors a plethora of genotypes.[21],[22] A recent study suggests that core antigen levels are not influenced by mutations in the core region and the HCVcAg assay seems to identify genotypes 1-4 with equal sensitivity.[23] Another study among dialysis patients reported significant correlation between HCVcAg and HCV RNA levels across different HCV genotypes.[20] Of the 22 samples that were genotyped in this study, all the patients were positive for HCVcAg. There seems to be no discrepancy between genotype and HCVcAg positivity. Even though genotype did not seem to affect the core antigen levels ( P =0.335), a larger number of samples from this region need to be tested to understand the relationship between HCVcAg and different HCV variants. This assay presently shows a potential to detect the most prevalent genotypes in India i.e, genotypes 1 and 3. In summary, this technique provides smaller laboratories with the capacity to detect active HCV infection comparable to RNA detection techniques, thereby improving the monitoring of patients who are infected with HCV. Acknowledgement We thank Ortho Clinical Diagnostics India Ltd for providing the HCV core antigen kits (trak-C). References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07010f2.jpg] [mb07010f1.jpg] [mb07010t1.jpg] [mb07010f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}