 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
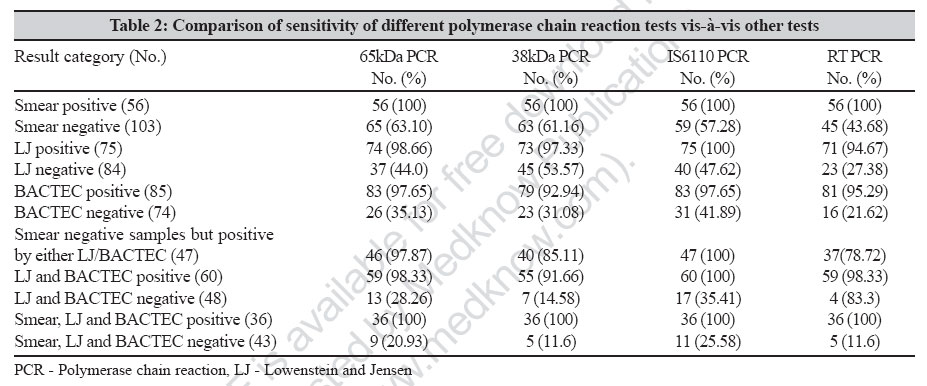
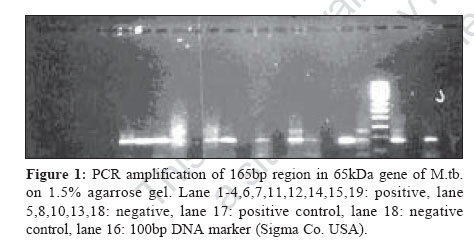
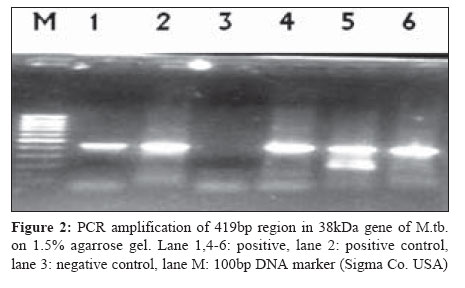
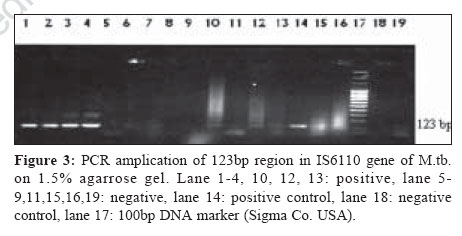
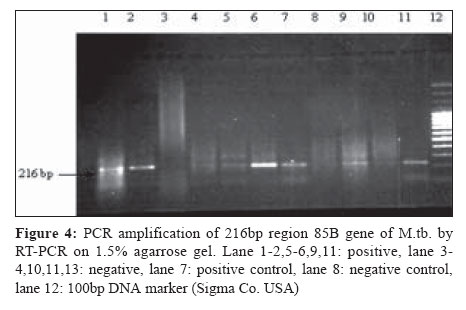
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 43-49 Original Article Diagnostic potential of IS6110, 38kDa, 65kDa and 85B sequence-based polymerase chain reaction in the diagnosis of Mycobacterium tuberculosis in clinical samples Negi SS, Anand R, Pasha ST, Gupta S, Basir SF, Khare S, Lal S Tuberculosis Laboratory, Microbiology Division, National Institute of Communicable Diseases, New Delhi - 110 054 Date of Submission: 28-Nov-2005 Code Number: mb07011 Abstract Purpose: The correlation between the presence of specific gene sequence of M. tuberculosis and specific diagnosis of clinical tuberculosis is not known. This study compared the results of polymerase chain reaction (PCR) amplification of M . tuberculosis specific DNA sequences (IS6110, 65kDa, 38kDa and mRNA coding for 85 B protein) from different clinical samples of pulmonary and extrapulmonary tuberculosis.Methods: One hundred and seventy-two clinical samples from suspected tuberculosis patients were tested for smear examination, culture (LJ and rapid BACTEC 460 TB system) and PCR. PCR was performed with specific primers for the targets: IS6110, 65kDa, 38kDa and 85B. Results: Each PCR test was found to have a much higher positivity than conventional test and BACTEC culture ( P <0.05). Smear positive samples (56) and the samples (36) showing positive results by conventional methods (smear and LJ medium culture) and BACTEC were found to be positive by all PCR protocols. No significant difference was found between the four PCR protocols ( P >0.05). The primer specific for amplifying the 123bp IS6110 fragment gave the highest positivity (83%), followed by 65kDa, 38kDa and 85B RT-PCR in descending order. Conclusions: These data suggest that the presence of IS6110 correlates more closely with the diagnosis of clinical tuberculosis than that of 65kDa, 38kDa and 85B proteins. Keywords: M. tuberculosis, polymerase chain reaction, IS6110, 65kDa, 38kDa, 85B RT-PC Polymerase chain reaction (PCR) for M . tuberculosis has already proven to be a useful tool for the diagnosis of tubercular infection. However, the use of PCR in the detection of M. tuberculosis has produced varying results especially in relation to the sensitivity of the test.[1],[2],[3] Several M . tuberculosis specific target DNA sequences have been used and these include gene coding for the 65kDa heat shock protein (HSP), IS6110 insertion sequence, gene coding for 38kDa only, 85B antigen and 16S rRNA for diagnosis by PCR and various other genotypic methods.[4],[5],[6],[7],[8],[9] Most of the PCR studies have targeted IS6110 sequence of M . tuberculosis genome because of the presence of repetitive sequence of IS6110 gene.[5],[10],[11] This characteristic helps to increase the sensitivity of PCR over that obtained in the amplification of single DNA sequence.[11] However absence or the presence of very few copies of this sequence have already been reported in some strains of M . tuberculosis .[12],[13],[14],[15] Therefore, the present study was designed to evaluate the potential of four different M . tuberculosis specific DNA sequences (IS6110, 65kDa, 38kDa and mRNA coding for 85 B protein) in various clinical samples from suspected cases of tuberculosis. Materials and Methods Clinical specimens One hundred and seventy two clinical samples were obtained with a strong clinical/ radiological/ histopathological evidence of TB (both pulmonary and extrapulmonary) including clinical response to antitubercular treatment referred from different hospitals of Delhi like LNJP (Lok Nayak Jai Prakash), GTB (Guru Teg Bahadur), KSC (Kalawati Saran Children), AAA (Aruna Asaf Ali) hospitals in the year 2003. These criteria were used as gold standard for classifying cases of TB. All the necessary clinical details were obtained from the referring hospitals in the prescribed format provided by us. The samples included 57 sputum, 30 pus, 23 skin biopsies, 18 BAL (Broncho alveolar lavage), 18 synovial fluid and synovial tissue, six urine (UTI), four lymph node aspirates, five CSF, three other biopsies, three menstrual blood, one sample each of pleural fluid, bone marrow aspirate, ascitic fluid, endometrial biopsy and semen. In addition, 37 sputum samples obtained from nontuberculous individuals (chronic asthmatics, chain smokers) initially screened by AFB smear examination and chest X-ray, were also used in the study as negative controls. Inclusion criteria All the new suspected cases of tuberculosis of either sex and all age groups having a strong clinical/radiological / microbiological evidence of tuberculosis and not receiving antitubercular treatment for more than four weeks were included in the study. Exclusion criteria Smear negative patients with pulmonary and extrapulmonary TB not responding to ATT even up to eight weeks of treatment were excluded from the study. Processing of samples for culture All the samples were processed in the Microbiology department of National Institute of Communicable Diseases (NICD), Delhi, India. For every clinical sample, smear microscopy and culture on both LJ and BACTEC 12B media were done as described earlier.[3] The mycobacterial isolates obtained in culture were subjected to limited biochemical testing for species characterization by carrying out Niacin test (commercially supplied Niacin strip by Sigma were used) and NAP sensitivity test (Becton Dickinson, USA) as described earlier.[3],[16] Polymerase chain reaction Processing of samples The deposits of the clinical samples obtained after processing with NALC- NaOH and other appropriate method described earlier[3] were used for DNA and RNA extraction which were then used for amplification of various gene sequences by PCR. DNA was extracted using commercially available QIAmp DNA kit, QIAGEN company, Germany with one initial additional step. The preliminary processed materials as described above were kept at 80°C for 10 min for inactivation of possible mycobacteria. The material was then further processed as per the guidelines of the manufacturer of the kit to obtain the DNA. RNA was extracted from the clinical sample as described earlier.[7] All DNA and RNA sequences were amplified in a PCR thermal cycler model 2700 (Applied Biosystems). Amplification of the 65kDa antigen coding gene (165bp) of M. tuberculosis Amplification of the 165bp sequence of the 65kDa HSP antigen was done as described earlier.[3] Amplification of the 38kDa gene (419bp) of M . tuberculosis . The 419bp sequence of the 38kDa gene was amplified using primes Pabf (5′- ACCACCGAGCGGTTCGCCTGA-3′)and Pab r (5′- GATCTGCGGGTCGTCCCAGGT -3′).[17] Briefly, a 25 µL reaction was set up containing 10.7 µL of double distilled H2O, 2.5 μL of 10X buffer, 1.5 μL of 25 μM MgCl2, 300 μM (each) of the four deoxyribonucleoside triphosphate (available in Gene Amp PCR core reagent kit supplied by Applied Biosystem of Roche Company, USA), 2.5U of Taq polymerase (Perkin Elmer), forward and reverse primer at final concentration of 10 pmol and 5 μL of DNA sample. The following amplification cycle was used for PCR: Three min at 95°C, 30 cycles each of one min at 94°C, one min at 63°C and 72°C for one min followed by one cycle of 72°C for one min-. Amplification of the IS6110 gene (123bp) of M. tuberculosis DNA amplification of the 123bp IS6110 insertion element was carried out by two oligonucleotide primers IS6110f (5′- CCT GCG AGC GTA GGC GTC GG-3′) and IS6110 r (CTC GTC CAG CGC CGC TTC GG-3′).[11] Briefly, a 25 μL reaction was set up containing 10.7 μL of double distilled H2O, 2.5 μL of 10X buffer, 1.5 μL of 25 μM MgCl2, 300 mM (each) of the four deoxyribonucleoside triphosphate (available in Gene Amp PCR core reagent kit supplied by Applied Biosystem of Roche Company, USA), 2.5U of Taq polymerase (Perkin Elmer), forward and reverse primer at final concentration of 10 pmol and 5 μL of DNA sample. The following amplification cycle was used for PCR: five min at 94°C, 30 cycles each of one min at 94°C, one min at 63°C and 72°C for one min, followed by one cycle of 72°C for seven min. Amplification of 216bp region of mRNA coding for 85B antigen by RT-PCR The 216 bp sequence of the mRNA coding for 85B protein of the 85B antigen complex was amplified using two set of primers.[7] MRL41
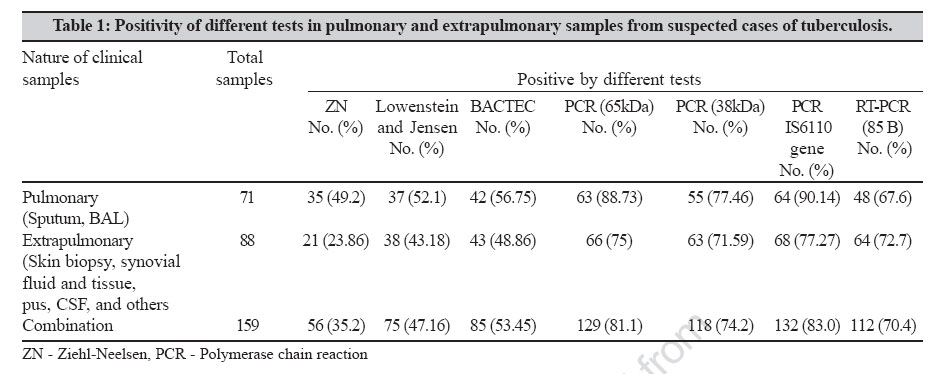
GAG TAC CTG CAG GTG CCG TCG CCG TC STN RT-PCR was performed as described below: RT-PCR was done with a final volume of 20 μL containing 0.8 μM antisense outer primer (MRL42), 200 μM dNTP (each), 2 μL 10X Buffer 1.2 μL MgCl2 (25 mM/1.5 mL), RNase inhibitor (1U), 2.5 U of MuLV reverse transcriptase (all Perkin-Elmer) and 4.5 μL of extracted RNA. To initiate synthesis of cDNA, this reaction mixture was kept at 60°C for 30 min, followed by 94°C for two min-. Ten microlitre of cDNA were added to 40 μL of PCR reaction containing 5 μL 10X Buffer, 3 μL MgCl2, 5 Unit of Taq DNA polymerase (all Perkin Elmer), 0.8 μM outer sense primer (MRL41) and distilled water to carry out outer RT-PCR. The thermal cycling condition used were 30 cycles of denaturation at 94°C for 45 sec, with primer annealing and extension carried out in one step at 70°C for one-five min. Inner PCR was then performed by using 1.5 μL of outer PCR product, 2.5 uL 10 X buffer, 1.5 µL MgCl2, 200 µM dNTP, 2.5 U Taq DNA polymerase and inner primer (MRL 43 and 44) at a concentration of 0.8 µM and rest distilled water to make the final volume 25 µL. Thermal cycling included 30 cycles of denaturation at 94°C for 45 seconds, primer annealing at 60°C for 45 seconds and extension at 72°C for 45 seconds, after which the reaction mixture were held at 72°C for 10 min.. All PCR protocols were modified from earlier described protocols, as we were unable to obtain consistent results with our positive controls using previously described protocols. Each PCR experiment was carried out with positive control (H37Rv strain of M. tuberculosis ) and negative control (double distilled water). Gel electrophoresis of amplified DNA and RNA Amplified DNA was electrophoresed in 1.5% agarose gel whereas amplified RNA was electrophoresed in 3% agarose gel at 100V for half an hour and visualized under ultraviolet light after staining the gels with ethidium bromide. Statistical analysis Results were analyzed to determine concordance between conventional test (Smear examination and LJ medium culture), rapid BACTEC culture and PCR and also among the four PCR protocols used, by F test. Results Initially, 172 clinical samples with strong clinical suspicion of tuberculosis were subjected to all the tests discussed. Out of these, 13 samples were contaminated in BACTEC culture (6.4%) and of these 13 samples, 12 samples were also found to be contaminated in LJ media (5.8%). Accordingly, in this study, we compared the results of 159 samples only. In addition, 37 sputum samples obtained from nontuberculous subjects used as negative control were also analyzed. Overall results are summarized in [Table - 2][Table - 2] while the [Figure - 1][Figure - 2][Figure - 3][Figure - 4] show the amplified product of the four PCR protocols used. [Table - 1] depicts the positivity of different tests performed in both pulmonary and extrapulmonary samples individually as well as in combination. As evident from [Table - 1] each PCR test was found to have a much higher positivity than conventional test and BACTEC culture ( P < 0.05), though positivity differs in each PCR. PCR targeting 165bp region of 65kDa antigen coding gene showed a sensitivity of 81.1% followed by PCR targeting 38kDa, IS6110 and mRNA coding for 85 B protein showing sensitivity of 74.21, 83.0 and 70.4% respectively. For specificity all the tests described were performed in 37 confirmed negative samples. ZN stained smear examination, LJ and BACTEC cultures were found to be 100% specific. On the other hand none of the PCR tests were found to be 100% specific. PCR targeting 65kDa, 38kDa, IS6110 and 85B were found to be 94.59, 97.29, 94.59 and 89.18% specific by showing false positivity in 2, 1, 2 and 4 samples respectively (data not shown). Pulmonary samples Of the 71 samples from pulmonary TB cases, 35 (24 sputum and 11 BAL) were positive for AFB smear examination (49.29%). Of the 71 pulmonary samples, 37 (57.11%, 25 sputum and 12 BAL) were positive for M . tuberculosis growth on LJ media while in case of BACTEC system, 42 (33 sputum and 9 BAL) samples were positive for M . tuberculosis (56.75%). PCR targeting IS6110 gene showed highest positivity and was able to detect mycobacterial DNA in 64 samples (50 sputum and 14 BAL) followed by the one targeting 65kDa antigen-coding gene showing positive results in 63 samples (50 sputum and 13 BAL). PCR targeting gene for 38kDa antigen showed positive result in 55 samples (45 sputum and 10 BAL). RT-PCR was found to be least sensitive [Table - 1] by showing the positive result in 48 samples only (41 sputum and 7 BAL). Extrapulmonary samples Of the 88 samples from extrapulmonary TB cases, only 21(23.86%) were found to be AFB positive by smear examination. LJ medium culture detected M . tuberculosis growth in 38 (42.18%) samples whereas BACTEC culture positivity was found to be slightly higher i.e., in 43 (48.63%) extrapulmonary samples. PCR amplifying 123bp region of IS6110 showed the sensitivity of 77.27% followed by PCR targeting 65kDa, mRNA coding for 85B protein and 38kDa showing the sensitivity of 75, 72.7 and 71.59% respectively, though the difference was not found to be statistically significant ( P < 0.05). All the conventional tests and PCR tests targeting different regions showed higher rate of detection in pulmonary samples than in extrapulmonary samples, though the difference was not found to be statistically significant ( P >0.05). All the culture isolates obtained were confirmed as mycobacteria with the biochemical tests discussed. We also tried to compare the positivity of PCR tests targeting different genes i.e., 65kDa, 38kDa, IS6110 and 85 B RT-PCR vis-à-vis three different tests i.e, Smear examination, L J culture and BACTEC culture results individually as well as in combination [Table - 2]. The positivity of detection of M . tuberculosis in AFB smear positive samples by all PCR tests approached 100%. In other clinical samples that were negative by smear examination, PCR presented inconsistent results depending on the primers used. In smear negative specimens PCR targeting 65kDa coding gene showed a highest positivity of 63.1% in comparison to other target genes. IS6110 based PCR showed the positivity of 100% in clinical samples, which were found positive in LJ media. On the other hand, PCR targeting 65kDa, 38kDa and 85B antigen showed 98.66, 97.33 and 94.67% positivity. Similarly, 97.65% positivity was observed by 65kDa and IS6110 PCR in clinical samples which were positive by BACTEC culture followed by 38kDa and 85B antigen PCR showing 92.94 and 95.29% positivity respectively. IS6110 PCR showed a positivity of 100% for the clinical samples, which were positive for M . tuberculosis by both the culture methods used followed by PCR targeting 65kDa and RT-PCR showing a positivity of 98.33%. All PCR protocols targeting 65kDa, 38kDa, IS6110 and 85B protein antigen coding gene showed 100% positivity for clinical samples which were positive by all the other three methods used (ZN, LJ and BACTEC). Even in 43 samples negative by all the other three tests used, IS6110 PCR test was able to detect 11 positives (25.58%) and these were not likely to represent false positive result as PCR was repeatedly positive on these sample and further these samples were collected from highly suspected cases of tuberculosis who responded positively to the antitubercular treatment [Table - 2]. In 28 samples (21 extrapulmonary and seven pulmonary) PCR test was found positive by one or other PCR protocols whereas all other conventional and BACTEC tests were negative (data not shown). The mean detection time for M . tuberculosis was 24.03 days by LJ media culture, 12.89 days by BACTEC and less than one day by smear examination and PCR test targeting IS6110, 38kDa, 65kDa. However, the mean detection time for M . tuberculosis was two days by RT-PCR targeting 85 B. Discussion In the present study, we evaluated and compared four PCR protocols involving four different M . tuberculosis specific DNA sequences i.e., IS6110 gene, 38kDa and 65kDa antigen coding gene and 85B mRNA sequence for the early diagnosis of tuberculosis in pulmonary and extrapulmonary clinical samples and thus develop a rapid specific and sensitive PCR test based on the amplification of the genes cited in this study. The utility of the objective lies in the fact that delay in reaching a confirmatory diagnosis of tuberculosis result from the slow growth of the Mycobacterium species and early diagnosis of tuberculosis helps in early treatment and thus preventing the possible transmission of the infection. The high sensitivity of the PCR raises hope for more rapid diagnosis of these infections. The oligonucleotide primers derived from IS6110 gene, Pab DNA sequence of 38kDa and 65kDa heat shock protein and mRNA coding for 85 B protein were successfully used to amplify a 123bp, 419 bp and 165bp DNA sequence and 216bp mRNA coding for 85B protein in mycobacteria belonging to the M . tuberculosis complex, but not in other species. The primers we used were highly specific for each DNA sequence and were selected because they had been used by others. The four PCR protocols were conducted on 159 clinical samples and the results were compared with those obtained by conventional methods. All the four PCR methods correlated well in both specificity and sensitivity with the conventional methods. Additionally, it showed usefulness not only for patients with positive results by the conventional methods but also for 28 samples (21 extrapulmonary samples and seven pulmonary samples) that were negative by the conventional methods. These 28 samples included seven pus, six skin biopsy, five BAL, two samples each of sputum, lymph node aspirate and urine, one sample each of pleural fluid, cerebrospinal fluid, menstrual blood and endometrial biopsy. Our results showed that the four PCR protocols detected TB in various pulmonary and extrapulmonary specimens with highest positivity by IS6110 gene-based PCR followed by 65kDa, 38kDa and 85B in descending order but the difference was not found to be significant (p< 0.05). The only possible reason could be presence of multiple copies of IS6110 sequence in the M . tuberculosis genome whereas other target genes were present in single copy. Our result of higher positivity of IS6110 gene based PCR is also supported by earlier studies. Lee et al[18] showed better result by IS6110 gene based PCR on comparison with 65kDa and MPB 64 PCR in diagnosis of tuberculous meningitis. Ogusku et al[19] showed highest positivity by IS6110 gene based PCR (92.1%) on comparing with specific primer targeting 65kDa, 38kDa and MPB 64. The major advantage with these different PCR protocols was their extreme sensitivity though false positive result were shown by each PCR test used. Similar problems with regard to false positive results were reported by earlier studies.[5],[18],[19] The possible explanation for false positive results may be cross contamination of template DNA which could not be detected by the other protocols or cross reaction with other target DNA besides M . tuberculosis .[20] All false positive results seen with different PCR protocols in negative control samples indicate that cross contamination with TB DNA was the most likely cause. The percentage of positivity for the amplification of the 123-bp fragment of target IS6110 in the present study (83.0%) was higher than that reported by Nolte et al[21] and Montenegro et al ,[2] who obtained 57.0, 53.0 and 76.7% respectively. However, our result of 83% positivity in IS6110 PCR was less than that of Ogusku et al[19] showing 92.1% positivity. Using 65kDa primers, positivity of the PCR was 81.1% which was more than that of Ogusku et al[19] showing 76.3% positivity by the 65kDa PCR and Pierre et al[22] reported only 40% positivity by the 65kDa PCR. As for 38kDa primers, positivity was 74.2%, lower than the 86.8% reported by Ogusku et al ,[19] 85.5% reported by Dwivedi et al[23] and higher than Sjobring et al[17] showing 42.85% positivity. As for mRNA primer coding for 85B protein, positivity was 70.4% lower than the 83% reported by Jou et al .[7] Our positivity rates of 90.14 and 77.27% in pulmonary and extrapulmonary samples was also higher than that of Tiwari et al[5] showing 75.67 and 61.7% positivity by PCR amplifying 123bp region of IS6110 in pulmonary and extrapulmonary samples of tuberculosis. We also compared our different PCR protocols results vis a vis three different test i.e., smear examination, LJ culture and BACTEC culture, individually as well as in combination. In the smear positive category all PCR protocols showed 100% positivity. This observation was comparable to Ogusku et al[19] showing 100% positivity by PCR targeting IS6110, 65kDa and 38kDa, in smear positive samples. In the smear negative category, 65kDa PCR showed the highest positivity of 63.10% followed by 38kDa IS6110 and RT-PCR showing 61.16, 57.28 and 43.66% positivity respectively. Our result of 63.10% positivity by 65kDa PCR was slightly higher than our earlier published study by showing 62.5% positivity by 65kDa PCR in smear negative samples. Dwivedi et al[23] showed 76.36% positivity of 38kDa PCR in smear negative samples. Tiwari et al[5] showed 55% positivity of IS6110 PCR in smear negative samples. Jou et al[7] showed 83% sensitivity by RT PCR targeting m RNA coding for 85 B protein in smear negative samples. In LJ culture positive samples only IS6110 PCR showed 100% positivity followed by 65kDa, 38kDa and 85B protein PCR showing 98.66, 97.33 and 94.67% positivity. In BACTEC positive samples, none of the PCR methods achieved 100% positivity. Two samples, one of endometrial biopsy and the other of synovial fluid, showing the positive BACTEC result, showed negative results by all the PCR tested. In LJ and BACTEC culture positive category, once again only IS6110 PCR showed 100% positivity. Our results of different PCR in culture positive samples was also supported by earlier studies. Pao et al[4] showed the 100% positivity by 65kDa PCR in culture positive samples. Dwivedi et al[23] showed 100% positivity by 38kDa PCR in culture positive samples of sputum. Clarridge et al[10] showed 83% positivity by IS6110 PCR in culture positive samples. Jou et al[7] showed 100% positivity by 85B mRNA PCR in culture positive samples. The differences in positivity percentages between the present study and those in the literature may be related to the slight changes in the adopted protocols, such as the sample decontamination processes and variation in the composition of lysis buffer solutions. PCR protocols described here also showed their utility by showing the positive result in culture negative samples of LJ and BACTEC in combination. Seventeen such samples were found where IS6110 PCR showed amplification of 123bp region of IS6110 gene. This was followed by 65kDa, 38kDa and mRNA 85B protein coded PCR showing 28.26,14.58 and 8.33% positivity in such samples. All culture negative but PCR positive specimens belonged to patients who had clinical signs indicative of tuberculosis including characteristic radiograph, typical clinical manifestations of the disease, positive exposure history or past history of tuberculosis and /or clinical response to antituberculosis chemotherapy. Further the positivity of various PCRs in culture negative samples was supported by earlier studies. Pao et al[4] showed 41.56% positivity by 65kDa PCR in culture negative samples. Dwivedi et al[23] showed 66.7% positivity by 38kDa PCR in culture negative samples. Clarridge et al[10] showed 1.16% positivity by IS6110 gene based PCR in this category samples. Lee et al[18] showed 33.3% positivity by PCR targeting IS6110, 65kDa and MPB 64 in culture negative samples. All PCR protocols in this study showed 100% positivity in the samples found to be positive by all the conventional tests used. In addition, in the 43 clinical samples showing negative result by all the conventional tests used, PCR targeting 123bp region of IS6110 showed positive result in 11 samples (25.58%) followed by 38kDa, 85BmRNA showing positive result in five samples (11.6%) and 65kDa showing positive result in nine samples (20.93%). These results are unlikely to be false positive as the patients from whom these samples were obtained gave a positive response to antituberculosis chemotherapy on follow up. Our study and those of others suggests that PCR could make a considerable impact in the early diagnosis of TB, particularly extrapulmonary TB, which can often be missed by conventional tests producing negative result or causes an unacceptable delay in diagnosis. In conclusion, PCR has a potentially important role in strengthening the diagnosis of TB especially targeting IS6110. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07011f4.jpg] [mb07011f2.jpg] [mb07011t1.jpg] [mb07011f1.jpg] [mb07011f3.jpg] [mb07011t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}