 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
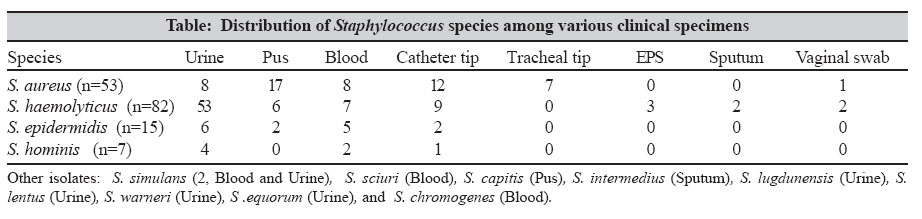
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 50-52 Brief Communications In vitro activity of antimicrobial agents against oxacillin resistant staphylococci with special reference to Staphylococcus haemolyticus Chaudhury A, Kumar AG Department of Microbiology, SV University of Medical Sciences, Tirupati - 517 507, Andhra Pradesh Date of Submission: 13-Nov-2005 Code Number: mb07012 Abstract One hundred and sixty seven isolates of staphylococci isolated from the inpatients of a tertiary care referral hospital in South India were speciated and activity of oxacillin, glycopeptides, linezolid and quinupristin/dalfopristin against these isolates was tested by broth microdilution method. Of the 114 coagulase negative staphylococci (CoNS), 49.1 % were S. haemolyticus, isolated predominantly from urine (64.6%), while the rest belonged to 11 other species. More than half the isolates of S. aureus (52.8%) and 68.4% of the CoNS were oxacillin resistant. All the strains were uniformly susceptible to vancomycin, linezolid and quinupristin/dalfopristin; but 25.6% isolates of S. haemolyticus showed reduced susceptibility to teicoplanin (MIC: 8-16 mg/L). Our study demonstrates the high prevalence of oxacillin resistance among hospital isolates of S. aureus and CoNS in India. Vancomycin, along with the newer agents like linezolid and quinupristin/dalfopristin remains the drug of choice for treating multi drug resistant staphylococcal infections.Keywords: Antimicrobial susceptibility, coagulase negative staphylococci, S. haemolyticus Staphylococcus aureus and the coagulase negative Staphylococcus species (CoNS) are among the most common causes of mortality and morbidity in the hospital setting worldwide. In 1995, Staphylococcus aureus was recovered from 13% of infections and ranked as the most common cause of nosocomial infection in the USA.[1] According to the most recent report from National Nosocomial Infections Surveillance, USA; S. aureus and CoNS constitute the most common nosocomial pathogens in both ICU and nonICU inpatient areas.[2] Given the importance of staphylococci in hospital setting, this study was done to find out the distribution of the various staphylococcal species in this hospital. The prevalence of oxacillin resistance among these isolates together with their susceptibility to glycopeptides and two newer agents (linezolid and quinupristin/dalfopristin) was also investigated. Materials and Methods A total of 167 consecutive staphylococcal isolates from various clinical specimens from the inpatients of a tertiary care hospital in India, were included in the study. Preliminary identification was done by colony character, Gram stain and slide coagulase test. Speciation was done first by manual conventional test followed by definitive identification with Vitek ID 32 Staph (Version 2-0); (bioMιrieux, Durham, NC, USA). β -lactamase production was tested by nitrocefin disk (Becton Diskinson, Cockseyeville, MD, USA). Minimum inhibitory concentration (MIC) test was performed by the NCCLS broth microdilution technique for oxacillin, vancomycin, teicoplanin, linezolid and quinupristin/dalfopristin.[3] S. aureus ATCC 29213 was used as the reference strain for the broth dilution technique. Results Fifty-three (31.7%) of the strains were S. aureus while the remaining 114 (68.3%) belonged to various species of CoNS. Twelve different species were identified among the CoNS, of which S. haemolyticus was the most frequent isolate (82, 49.1%). [Table - 1] shows the source of the isolates and the species distribution. The majority of the S. haemolyticus isolates were from urine (53/82, 64.6%). Antimicrobial resistance was found to be widespread among the isolates, with 142 strains (85.0%) showing β -lactamase production. A total of 106 strains (63.5%) were oxacillin resistant; comprising 52.8% of S, aureus (MIC ≥ 4 mg/L) and 68.4% of the CoNS (MIC ≥ 0.5 mg/L). About a quarter (25.6%) of the S. haemolyticus isolates showed intermediate sensitivity to teicoplanin (MIC: 8-16 mg/L), while the other isolates of CoNS and also of S. aureus were sensitive to this agent (MIC ≤ 8 mg/L). All the 167 strains of staphylococci included in the study were uniformly susceptible to vancomycin (MIC: 0.5-2.0 mg/L), linezolid (MIC: 1.0-2.0 mg/L) and quinupristin/dalfopristin (MIC: 0.25-1.0 mg/L). Discussion The prevalence of S. aureus and various species of CoNS in the hospital setting together with their susceptibility patterns have been reported in a number of studies.[4],[5] A few studies from India have also highlighted this problem along with prevalence of antimicrobial resistance of the isolates from health care settings.[6],[7] In our study, majority of the isolates were CoNS and almost half of these isolates (82/167, 49.1%) were S. haemolyticus . Some studies have shown similar findings with this species as the predominant isolate among the CoNS.[4],[8] Interestingly, of the 71 staphylococci isolated from urine, 53 (74.6%) were S. haemolyticus , making it the most common Staphylococus species involved in nosocomial urinary tract infection in this hospital setting. One previous study has reported similar finding, where the isolation rate of this organism was 47.8%.[4] In another study, S. haemolyticus was the predominant pathogen isolated from immunocompromised patients (45%).[8] These findings are alarming since there is high prevalence of multidrug resistance in S. haemolyticus , particularly to the glycopeptides.[9] This is due to the peculiar propensity of these organisms to develop resistance to glycopeptides in a single step upon exposure to these antibiotics.[9] In our study, reduced susceptibility to teicoplanin (MIC:8-16 mg/L) was noted among 25.6% of the S. haemolyticus strains and not among the members of other species. Reduced susceptibility or resistance of staphylococci particularly S. haemolyticus for the glycopeptide antibiotics has not been addressed adequately in Indian studies. In the international multi-centre study RESIST in 1997 and 1998,[5] resistance to teicoplanin was significant among methicillin resistant strains of CoNS, particularly among S. haemolyticus . In our study, all the strains of Staphylococcus species were uniformly sensitive to vancomycin. Methicillin resistance among staphylococci is widespread in India. In a multicentre study from India in 1996,[7] prevalence of MRSA ranged from 27% in Bombay to 47% in Bangalore and 42.5% in Delhi. A study from Eastern India in 2001 revealed 66.6% of S. epidermidis and 60% of S. haemolyticus strains resistant to oxacillin.[6] The most recent data from India gives a figure of 66% methicillin resistant CoNS among neonatal septicaemic patients; isolated from blood and skin of these patients.[10] As revealed in the present study, our hospital has a prevalence rate of 52.8% of oxacillin resistant S. aureus and 68.4% of oxacillin resistant CoNS. These rates approximate the figures from India.[6],[7],[10] In the most recent report from USA in 2004, the average prevalence of MRSA was 48.1% and 44.9% from ICU areas and non ICU areas respectively; while the corresponding figures for CoNS was 76.3% and 65.2% respectively.[2] Our figures correspond roughly to the USA data as well. Among the newer anti-staphylococcal agents, all the strains in our study were sensitive to linezolid and quinupristin / dalfopristin. A large scale study with these two agents have found them to be highly active against all isolates of Staphylococcus species, regardless of their resistance to other agents.[11] However, one study has found 15 out of 658 (2.3%) isolates of CoNS being resistant to quinupristin/dalfopristin.[12] Ever since its introduction in 1984, vancomycin had stood the test of time as the last resort in treating multidrug resistant staphylococcal infections, particularly those caused by methicillin resistant strains. This reliability on vancomycin has been shaken in the last few years with isolated reports of vancomycin resistance, which first originated from Japan and later on from USA and Europe. The emergence of S. aureus strain that are hetero-intermediately resistant to vancomycin (hVISA) has been reported recently originating from various Asian countries including India.[13] To counteract this potential threat, newer agents like linezolid, daptomycin and quinupristin/dalfopristin have come into use. These agents, till now, have shown excellent activities against both S . aureus and CoNS. Nonetheless, with the increasing use of these agents, we may encounter resistance to these drugs in future. It is important that large referral hospitals, particularly in countries like India, keep a continuous surveillance on the antimicrobial susceptibility pattern and the clinicians use these new agents judiciously to prevent antimicrobial resistance. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07012t1.jpg] |
| |||||||||
{kind=link}