 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
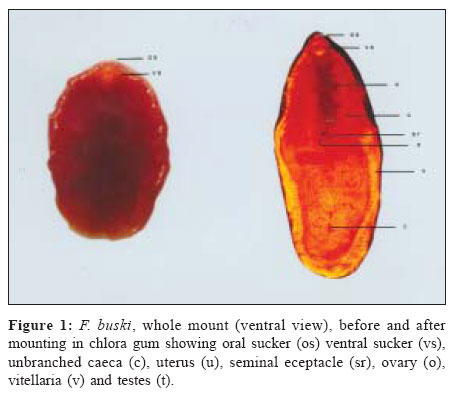
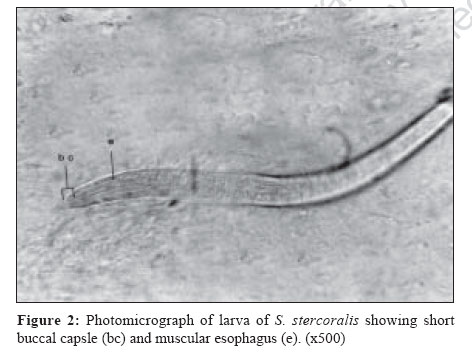
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 62-63 Case Report A case of poly-parasitism involving a trematode and four different nematodes in a migrant from Bihar Rai S, Wadhwa V, Kharbanda P, Uppal B Maulana Azad Medical College and LN Hospital, New Delhi - 110 003 Date of Submission: 04-Jun-2005 Code Number: mb07005 Abstract Reported is a case of seven-year-old, migrant from Bihar state, infested with Fasciolopsis buski Strongyloides stercoralis Ascaris lumbricoides , Trichuris trichiura and Ankylostoma duodenale in feces. Patient responded to treatment with piperazine, thiabendazole and albendazole, the importance of considering multiple and non-endemicparasite infestations in migrant of poor socio-economic background is emphasized.Keywords: Fasciolopsis buski, polyparasitism Parasitology is an important exception to the rule of single unifying diagnosis, especially in tropics where multiple infestations occur commonly in the gastrointestinal tract.[1],[2] F. buski , the giant intestinal fluke of man and pigs, is found in the South-East Asian countries including India.[3] Adult worm inhabits the gastrointestinal tract, commonly duodenum and jejunum. The eggs released in feces embryonate and hatch in water, releasing miracidia, which infect snails of Planorbidae family. The snails shed cercaria that encysts on surface or acquatic plants, debris and on water surface.[4] Ingestion of the cyst leads to infection, which presents as diarrhea, malnutrition and in severe cases, ascitis and death.[5] S. stercoralis infection is endemic in tropical countries. The infection remains asymptomatic in healthy individuals but can lead to hyper-infection syndrome in a compromised host. A. lumbricoides , though less harmful to the gastrointestinal mucosa, has migratory behavior and can cause obstruction in the gastrointestinal lumen. The present case describes a unique co-infection of a trematode with four different nematodes. Case Report A seven-year-old male presented with complaints of abdominal pain, vomiting (non-bilious) and diarrhoea (15-16) of two days duration. There was history of passing worms, resembling Ascaris , in vomitus and feces on two occasions earlier. After admission the patient vomited a red, dorso-ventrally flat, contractile leaf like worm. The family had migrated from Bihar four months back where the child used to bathe and play in pond. There was no history of intake of edible water plants. On examination, child was emaciated, weighing 16.2 kg (third percentile), afebrile, pale dehydrated and had no cyanosis or icterus. Vitals were stable. Systemic examination, USG abdomen and Chest X-ray were normal. Blood, stool and vomited worm were sent for laboratory examination. The patient was started on iv fluids. Laboratory results revealed: Hb; 10.2 g/dL, TLC; 6400/mm 3, DLC; P67 L32 E1. LFT were normal. Montoux test, serology for HIV, Leishmania, Echinococcus and Taenia were non-reactive. Immunoglobulin profile showed elevated levels of IgG (3033 mg/dL), IgA (312 mg/dL) and IgM (301 mg/dL). Separate estimation of IgE could not be carried out. The unsegmented parasite measured 4 cm x 2 cm. The trematode [Figure - 1] had an inconspicuous cephalic cone and two suckers (oral and ventral). The parasite was kept in chloral gum medium (for clearing) for 24h due to unavailability of the dyes used to stain the parasite. A subsequent examination showed; two suckers oral sucker and the ventral sucker (os and vs respectively), unbranched caeca (c), uterus (u), seminal receptacle (sr), ovary (o), vitellaria (v) and testes (t). The trematode was identified as F. buski. The feces was green, had undigested food particles and mucus. There were no worms or segments. A direct examination revealed larvae (33,000/gm), which measured 293 mx 17 m, had short buccal capsule (bc), muscular esophagus (e) and a pointed tail. They were identified as rhabditiform larvae of S. stercoralis [Figure - 2]. The examination also revealed eggs of A. lumbricoides, T. trichiura and A. duodenale (1000/gm each). Aerobic culture did not reveal any pathogen. Subsequently the patient was given piperazine (1.1 gm single dose), thoabendazole (760 mg for three days) and albendazole (200 mg single dose). The symptoms subsided after three days. A subsequent examination of feces revealed dead larvae of S. stercoralis (2000/gm). No ova, cyst or any undigested food particles could be seen. The patient left against medical advice and was lost to follow-up. Discussion Multiple parasitic infestation have become common as a result of improvements in laboratory diagnosis and growing population of immunocompromised indiviuals.[1] Mixed helminthic intestinal infestations are frequent in tropics, most frequent being co-infection of A. lumbricoides, T. trichiura and A.duodenale .[1] Reported is a unique case of poly-parasitism, which occurred in a seven-year-old migrant from Bihar, infesting agents included F. buski and S. stercoralis, A. lumbricoides, T. trichiura and A. duodenale. F. buski infestation has been reported in India from Assam, Bengal, U.P. and Maharashtra but this is the first reported case from a migrant from Bihar.[6],[7],[8] Diagnosis was made on the detection of adult worm in vomitus, which may have been triggered by migratory ascariasis evident from the patient history, whereas the mainstay is detection of eggs in feces. S. stercoralis infection was limited to the gastrointestinal tract as evident from the history, examination and absence of the filariform larvae in stool. Infestation with T. trichiura and A. duodenale is common in tropics and is considered for treatment after estimation of worm burden (significant counts being 2500/gm and 30,000/gm). The case emphasizes the need for strong suspicion of nonendemic infections and multiple etiologies in migrant population, as they are exposed to different endemic etiological agents. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07016f1.jpg] [mb07016f2.jpg] |
| |||||||||
{kind=link}
{kind=link}