 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
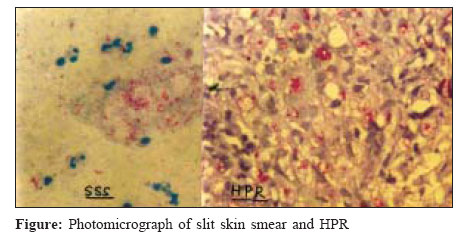
Indian Journal of Medical Microbiology, Vol. 25, No. 1, January-March, 2007, pp. 70-71 Case Report Lepromatous leprosy of histoid type Annigeri SR, Metgud SC, Patil JR Department of Microbiology, Jawaharlal Nehru Medical College, Belgaum - 590 010, Karnataka Date of Submission: 07-Jun-2005 Code Number: mb07019 Abstract Histoid leprosy is a variant of lepromatous leprosy, which develops as a result of resistance to dapsone monotherapy. Here we report two cases of lepromatous leprosy of histoid type, one with typical and another with atypical presentations.Keywords: Histoid, lepromatous leprosy Leprosy is a chronic granulomatous disease involving skin, peripheral nerves and nasal mucosa but capable of affecting any tissue or organ. Madrid classified leprosy into four types, lepromatous, tuberculoid, dimorphic and indeterminate.[1] Histoid lepromas are sudden eruptions of dome-shaped, tumors occurring in patients with lepromatous leprosy in association with dapsone resistance. These tumors resemble eruptive kerato acanthomas or cutaneous metastasis, since the first description of histoid lepromas by Wade in 1960, a number of similar patients have been observed and studied. We report here two cases of histoid leprosy, one with typical and another with atypical presentation. Case Reports Case 1 A 48-year-old man complained of raised lesions all over the body, which were itchy since six months, this complaint was accompanied by bleeding from nose since two months and pedal edema since eight days. There was no history of any altered sensation. Patient gave history of having itching all over the body three years back and had taken multi-drug therapy for leprosy for few months and discontinued it. On clinical examination multiple erythematous papules and plaques present over both forearms, elbows, neck, chest, abdomen and back. Few small lesions on face and lower limbs showed central indentation with excoriation and crusting, which were polymorphic in nature. Routine hematological investigations were normal. Bacteriological examination of slit skin smear revealed acid-fast bacilli of BI - 6+ and MI - 50-60%. Histopathology of nodules was done. Epidermis showed grenz zone and the dermis showed sheets of round to spindle histiocytes, compressing pilosebaceous apparatus. The nuclei were pyknotic and cytoplasm was foamy and vacuolated. Wade fit stain for lepra bacilli showed plenty of acid fast bacilli [Figure - 1]. These findings were suggestive of lepromatous leprosy of histoid type. He was treated with rifampicin, ofloxacin and minocycline (ROM) therapy initially and advised multi-drug therapy (MDT) for two years. Case 2 A 35-year-old lady, presented with nodules all over the body since 1½ years, which were covered with crusts. They were distributed more on the face, forearm, abdomen, back, buttocks and on the legs. Since last two months, the nodular lesions were associated with pain. This chief complaint was associated with epistaxis. She did not give any history of taking any antileprosy drugs. On clinical examination, the nodules were multiple, non-tender, firm to soft in consistency of size 0.5-3 cm papules present over the extensor surface of the forearm, dorsum of feet, abdomen, lower back, buttocks and thighs some of the nodules were ulcerated. The nasal bridge of the was collapsed. Routine blood examination was normal. Bacteriological examination of slit skin smear revealed acid-fast bacilli of BI-5.3 + MI - 60-80%. Histopathology of skin suggested lepromatous leprosy of histoid type. Discussion Histoid leprosy is not uncommon in south India. Histoid leprosy is considered a varient of lepromatous leprosy[2],[3] and by others as distinct entity.[4] There is male preponderance and the average age affected is between 21 and 40 years.[5] In India, its incidence among leprosy patients has been estimated to be between 2.79 to 3.60%.[5],[6] Initial report of histoid leprosy were associated with dapsone resistance and with relapse after dapsone monotherapy. However, this manifestation of leprosy has also been reported in patients in whom relapse occurred in presence of supervised monthly dose of multidrug therapy and in patients without any treatment.[2],[7] Histoid leprosy has characteristic clinical, histopathological and bacterial morphological features.[8] Clinically it is characterized by cutaneous and or subcutaneous nodules and plaques on apparently normal skin.[4] The lesions are usually located on the posterior and lateral aspects of arms, buttocks, thighs, dorsum of hands and on the lower part of the back[9] and over the bony prominences, especially over the elbows and knees.[10] Histopathologically the epidermis shows grenz zone and the dermis shows sheets of round to spindle shaped histiocytes. The nuclei are pyknotic and cytoplasm is foamy and vauolated. Wade fits stain for lepra bacilli shows plenty of acid fast bacilli. Histoid leprosy is managed by initially giving ROM therapy with rifampicin 600 mg. ofloxacin 400 mg, minocycline 200 mg once, which is followed by MDR therapy. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07019f1.jpg] |
| |||||||||
{kind=link}