 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
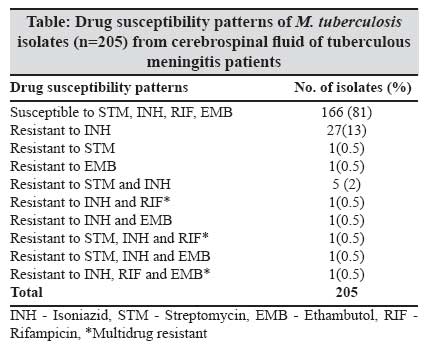
Indian Journal of Medical Microbiology, Vol. 25, No. 3, July-September, 2007, pp. 236-240 Original Article Comparative evaluation of bactec 460tb system and lowenstein-jensen medium for the isolation of M. tuberculosis from cerebrospinal fluid samples of tuberculous meningitis patients Venkataswamy MM, Rafi W, Nagarathna S, Ravi V, Chandramuki A Department of Neuromicrobiology, National Institute of Mental Health and Neurosciences, Bangalore - 560 029 Date of Submission: 29-Dec-2006 Code Number: mb07066 Abstract Purpose : To evaluate the role of the radiometric BACTEC 460TB system and the conventional Lowenstein-Jensen (LJ) medium for isolation of M. tuberculosis from cerebrospinal fluid (CSF) samples of tuberculous meningitis (TBM) patients. Keywords: BACTEC radiometric method, cerebrospinal fluid, Lowenstein-Jensen medium, sensitivity, tuberculous memingitis Tuberculous meningitis (TBM) is the most malignant form of neurotuberculosis. [1] Case fatality rate of untreated TBM is almost 100% and delay in treatment may lead to permanent neurological damage. [2] Microscopy by Ziehl-Neelsen (ZN) staining of cerebrospinal fluid (CSF) is positive in less than 10% of cases and isolation by using conventional solid media are associated with low sensitivity and is time consuming. The nucleic acid assays, owing to low sensitivity and high costs, are only an adjunct to and not the substitute for the conventional procedures. [3] The Centre for Disease Control and Prevention (CDC) Atlanta, Georgia, USA guidelines recommend that the laboratory identification of the M. tuberculosis complex be accomplished within 14-21 days after specimen collection. [4] Liquid media, as demonstrated by the radiometric BACTEC 460 TB system (Becton-Dickinson, Towson, MD) appear to be the best alternative for this purpose. It has evolved as the "gold standard" by which all other culture and detection systems are evaluated. [5] This system uses a selective broth medium containing C14-labelled palmitic acid, which improves recovery and decreases the time required for detection of mycobacteria. [6],[7],[8],[9],[10] The BACTEC mean detection time of M. tuberculosis in smear negative specimens has been reported to be better for tissues and fluids (14 days) than for respiratory specimens (24 days). [11] Recent recommendations for optimal recovery of mycobacteria from clinical specimens are to use a liquid medium along with one or more solid media, with Lowenstein-Jensen (LJ) slants being recommended as the primary medium. [12] Although the BACTEC 460TB system has been shown to be very useful in the diagnosis of pulmonary TB there are few published reports evaluating its role in the isolation of mycobacteria from extra pulmonary specimens, especially CSF specimens. We report the results of a study carried out to assess the utility of BACTEC radiometric method in the diagnosis of TBM in comparison with LJ medium and to determine the drug susceptibility testing of CSF isolates of M. tuberculosis . Materials and Methods Clinical specimens Culture procedures About 0.5-1 mL of CSF was added to the BACTEC 12B medium. As recommended, 0.1 mL of PANTA supplement (polymixin B 50 mg/mL, amphotericin B 5 mg/mL, nalidixic acid 20 mg/mL, trimethoprim 5 mg/mL and azlocillin 10 mg/mL. Becton Dickinson) was added to each BACTEC 12B vial prior to specimen inoculation. The culture media were incubated at 37°C, for six weeks. The BACTEC vials were tested for growth every two days during the first two weeks and weekly thereafter. BACTEC cultures showing a growth index (GI) ≥ 10 were read daily until the achievement of GI 50-100 and were subjected to Ziehl-Neelsen (ZN) stain and Gram stain. The vials, which remained negative for six weeks, were discarded. [13] A slope of LJ medium was inoculated with 0.25 to 0.5 mL of each specimen and incubated at 37 o C for eight weeks. The LJ slants were inspected weekly. Growth on the LJ slants resembling mycobacterial colonies i.e., rough, tough and buff-coloured, was subjected to ZN staining and Gram staining to confirm the presence of acid-fast bacilli and rule out contamination respectively. Identification Drug susceptibility testing Results Mycobacterial isolation Drug susceptibility Discussion This study was carried out to evaluate the utility of BACTEC 12B, in conjunction with the conventional LJ medium, in the early diagnosis of TBM. The sensitivity and rapidity of detection of mycobacterial growth in the CSF specimens from TBM patients was compared between the two different media and the role of BACTEC method in rapid drug susceptibility testing was also assessed. The data from this study shows that the rate of recovery of mycobacteria from CSF specimens by BACTEC radiometric method is far more superior as compared to the conventional culture on LJ medium. Moreover, the radiometric method is superior to the solid medium culture even in terms of rapidity in detection of growth. The recovery rates varying from 80 to 95% have been reported using BACTEC 12B whilst for LJ medium it varies from 42 to 77%. [12] The recovery rate in our study using BACTEC 12B was 93%, as against 39% by LJ medium. Thus the recovery rates in our study are consistent with observations from previous reports. [12] Among the total 2325 CSF specimens that were processed by both methods, 256 isolates grew in either media or both of them. Although 32% among these 256 culture positive specimens yielded growth in both the culture media, 61% were positive only in BACTEC 12B, which clearly demonstrates the enhanced sensitivity provided by this automated system in the laboratory diagnosis of TBM. There were 7% of the culture-positive specimens, which yielded growth only in the LJ medium. Therefore, there was no single medium, which could enable the detection of all the culture positive specimens. This suggests that some of the M. tuberculosis positive specimens may fail to yield growth if no additional solid medium is incorporated along with BACTEC 12B. Therefore the BACTEC system must be used concurrently with conventional culturing methods. [15] The reasons for some of the isolates which grew only on LJ and not in BACTEC 12B could be that these isolates were unable to metabolize the palmitic acid in this medium [16] or some of the growth promoting factors present in the egg-based medium may be absent in the BACTEC 12B medium. All the isolates belonged to the M. tuberculosis Complex as identified by the NAP differentiation test. In this study, only one additional solid medium was included with BACTEC 12B based on an earlier report, which compared the performance of BACTEC 12B, LJ medium and Middlebrookes 7H11 medium for isolation of mycobacteria from clinical specimens. The results of this earlier study suggested that there was no significant difference in the recovery of mycobacteria irrespective of whether an LJ slant or Middlebrooks 7H11 was used as an additional solid medium with BACTEC 12B medium. [10] Drug susceptibility test was performed by the BACTEC radiometric method for 205 CSF isolates of M. tuberculosis . The results were available within three weeks after identification of mycobacterial growth in the 12B medium by ZN staining. The drug susceptibility patterns suggest that most of the TBM cases are still caused by strains that are sensitive to anti tubercular drugs. Our data showed 80.98% of the clinical isolates to be sensitive to the first line drugs STM, INH, RIF and EMB. Therefore, by clinching an early diagnosis and with prompt treatment, it is possible to significantly bring down the high rates of mortality and morbidity associated with this dreaded form of extra-pulmonary TB. Resistance to INH was the most common (13.17%) single-drug resistance recorded which is consistent with earlier reports. Multi-drug resistance, i.e., resistance to INH and RIF, was observed in only three (1.46%) isolates, suggesting that MDR-TB is still not a confounding problem in the management of neurotuberculosis. However, with a tremendous escalation in the incidence of HIV-associated TB and recently reported incidence of TBM due to MDR strains, [17] it is essential to closely monitor the incidence of MDR-TB of CNS by regularly testing the drug susceptibility of the clinical isolates. In addition to the higher rate of recovery another significant advantage in using the BACTEC 12B was in terms of the time required for the detection of mycobacterial growth. The time for detection of growth by BACTEC method was twice as quick as that taken by LJ medium, an observation that is consistent with earlier reports. [11],[18] The BACTEC mean detection time of M. tuberculosis in smear-negative specimens was better for tissues and fluids (14 days) than for respiratory specimens (24 days). [11] The average time for recovery by BACTEC 12B was two weeks as against four to five weeks by LJ medium. In fact, many a times the isolation, identification and drug sensitivity testing was completed by the BACTEC method by the time growth could be detected on LJ medium. Another merit of BACTEC 12B medium was the lower number of specimens lost due to contamination i.e. 4% against a contamination rate of 10% on LJ medium. Therefore, the BACTEC 12B medium provides a tremendous advantage over LJ medium in terms of its rapidity in growth detection, increased sensitivity and a lower rate of specimens lost due to contamination. [19] Moreover, automated procedures carry the potential of introducing standardization in the mycobacteriology laboratory. [18] The biggest hurdle associated with the use of this method in a developing country is the initial investment and the recurrent costs that are involved. By facilitating early diagnosis, the BACTEC method may prove to be cost effective in a population with a high prevalence of tuberculosis, particularly in the extrapulmonary and paucibacillary forms of the disease. [6],[19] The importance of rapid detection and identification of mycobacteria for the management of TBM, which is the most malignant form of extrapulmonary TB, MDR-TB and HIV-associated TB, far outweighs the problems encountered due to cost constraints. However, the application of non-radioactive rapid culture systems, such as the mycobacterial growth indicator tube (MGIT), may prove to be more appropriate in the future for cost-effective TB diagnosis in developing countries. Acknowledgements MMV and WR acknowledge the Lady Tata Memorial Trust, Mumbai for providing the research fellowship. The authors acknowledge C. Basavaraju for technical assistance.References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07066t1.jpg] [mb07066f2.jpg] [mb07066f1.jpg] |
| |||||||||
![[Figure - 1]](/showimage?mb/photo/mb07066f1.jpg){kind=link}
![[Figure - 2]](/showimage?mb/photo/mb07066f2.jpg){kind=link}
{kind=link}