 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
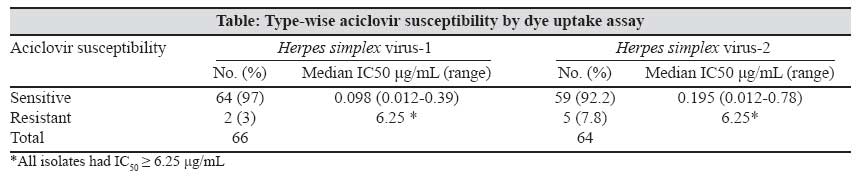
Indian Journal of Medical Microbiology, Vol. 25, No. 3, July-September, 2007, pp. 260-262 Brief Communication Aciclovir resistance among indian strains of Herpes simplex virus as determined using a dye uptake assay Abraham AM, Kavitha S, Joseph P, George R, Pillay D, Malathi J, Jesudason MV, Sridharan G Department of Clinical Virology, Christian Medical College, Vellore - 632 004, Tamil Nadu Date of Submission: 17-May-2006 Code Number: mb07072 Abstract Resistance to aciclovir (ACV) among Herpes simplex virus (HSV) isolates is increasingly being reported in the literature particularly in immunocompromised patients. However, there is only limited data available from India despite widespread use of ACV in our hospital. A cross-sectional study was hence conducted to determine the aciclovir (ACV) susceptibility of HSV 1 and 2 isolates using a dye uptake (DU) assay. This study showed a 3.0% prevalence of ACV resistance among HSV-1 strains (2/66, median IC 50 0.098 µg/mL) while in HSV-2 strains, it was 7.8% (5/64, median IC 50 0.195 µg/mL). The IC 50 for the HSV-1 and HSV-2 strains resistant to ACV was greater than or equal to 6.25 µg/mL.Keywords: Aciclovir resistance, dye uptake assay, Herpes simplex virus Herpes simplex virus-1 (HSV-1) and Herpes simplex virus-2 (HSV-2) are DNA viruses belonging to the Herpesviridae family that cause widespread infection in humans. Aciclovir (previously spelt acyclovir, ACV) was used from the 1980s in the treatment of HSV genital infections [1] and infections in the immunocompromised. [2] Since its first use, resistance to ACV has been reported from the West, particularly in immunocompromised patients [3] in whom the prevalence of resistant virus is typically 4 to 7% (compared to a mean of 0.3% in immunocompetent hosts). ACV has been used in India to treat HSV infections since the early 1990s. However, to our knowledge, only one study from India has been conducted that has reported ACV-resistance in vitro using a bioassay. [4] Apart from this study, no data is available regarding the ACV susceptibility of HSV isolates despite its widespread use in our population. In addition, there has been an increase in the number of patients with human immunodeficiency virus (HIV) infection or those undergoing immunosuppressive therapy for transplants. Hence, it was considered important to determine the pattern of susceptibility of HSV to ACV in patients in south India attending a tertiary care hospital. Materials and Methods This study was conducted at the Department of Clinical Virology of the Christian Medical College, Vellore between September 1998 and September 2004. The minimum sample size for this study (assuming a prevalence of 5% and with a desired precision of 4% [3] ) was estimated at 115 (CI: 95%) using Epi-Info Ver. 6.03 software. A total of 146 HSV isolates was obtained from clinical samples of 141 patients, seen in various units of the hospital (127 collected prospectively and 19 archived isolates stored from 1996). Another four isolates were obtained from Sankara Nethralaya, Chennai (of unknown ACV susceptibilities at the time of receipt). Standard and previously characterized ACV-resistant or -susceptible strains were obtained from Johns Hopkins Hospital (JHH), Baltimore, USA and Health Protection Agency (HPA), Colindale, London to verify the dye uptake (DU) assay used in the study. All samples were collected, transported and processed as described previously, [5],[6] inoculated into Vero, HEp-2 or A549 cells and identified using polyclonal (Dako A/S, Denmark) immunofluorescence assays (IFA) for HSV confirmation, followed by monoclonal IFA (Imagen Herpes simplex virus direct IF test, DakoCytomation, UK) for typing. A polymerase chain reaction (PCR) based on the pol gene was performed as described previously. [7] In the course of the study, 20 isolates were found to be non-cultivable and hence, a total of 130 isolates was available for testing. The titre of virus obtained from each sample was determined by a microtitre plate infectivity assay using the method of Reed and Muench. [5] Briefly, ten-fold serial dilutions of the test viruses were made in maintenance medium (MM) consisting of minimum essential medium (MEM) with 2% fetal calf serum (FCS) held on ice. Virus dilutions (10 -2 to 10 -7 ) were added to the appropriate rows after which Vero cells suspended in growth medium (GM) were added to all wells with appropriate cell controls. The plates were incubated in a CO 2 incubator at 37°C with 5% CO 2 for three days, during which the cell monolayer in each well of the microtitre plate was examined for the presence or absence of cytopathic effect (CPE). The method of Reed and Muench [5] was used to determine the 50% tissue culture infectious dose (TCID 50 ) on the third day. Subsequently, the neutral red dye uptake assay (DUA) was performed. The DUA is a quantitative colorimetric test based on the principle of preferential uptake of vital dye by viable cells over damaged cells. It was performed as described in a microtitre plate format. [8] Briefly, neutral red solution at pH 6.0 was added to each well after taking the visual reading. The plates were incubated for 45 min after which the dye was removed and the monolayer washed with pH 6.0 buffer. An elution buffer was then added to each well and gently rocked for 10 min to ensure even elution. Eluate in each well was transferred to an enzyme-linked immunosorbent assay (ELISA) plate in an exact template of the original microtitre plate and the OD of the wells was read using a spectrophotometer at 540 nm. Using the method of Reed and Muench, [5] the 50% dye uptake infectious dose (DU 50 ) endpoint was determined. The susceptibility of the isolates to ACV was determined using a method described previously [8] in a microtitre plate format with Vero cells and ACV IV (Zovirax by Burroughs Wellcome, Mumbai, India and Vir by Troikaa, Gujarat, India). Briefly, ACV IV 250 mg was reconstituted in sterile distilled water, aliquoted and stored at -20°C. When required, dilutions were made to obtain an in-use concentration of 25 µg/mL. Titrated HSV isolates were diluted in MM to give an in-use solution of 10-100 DU 50 /50 µL. In-use ACV solution was delivered and diluted serially to give concentrations ranging from 0.012 to 6.25 µg/mL (each drug concentration set up in 4 replicates). The respective virus dilutions were added followed by a Vero cell suspension. The plates were incubated in a CO 2 incubator at 37°C with 5% CO 2 for three days and examined for the presence or absence of CPE. After visual readings were taken, the neutral red DUA was performed as described previously. The 50% inhibitory concentration (IC 50 ) for each isolate was then determined (highest dilution of ACV that reduced CPE by 50%). The IC 50 was calculated by determining the mean OD obtained for each drug dilution (the highest dilution that had a mean OD less than that of cell controls was taken to be the IC 50 for that isolate) with threshold IC 50 values for resistance taken to be greater than 3.0 µg/mL [9] . Each assay was run with a standard susceptible and resistant strain respectively that had to perform satisfactorily for the run to be deemed valid. Results Of 141 patients whose samples yielded HSV, medical records showed that 50 (35.5%) were immunosuppressed, 19 (13.5%) were immunocompetent and there was no record of the immune status in 72 (51.1%). Fifty-five (39%) were not treated with ACV, 19 (13.5%) were previously treated with ACV and in 67 (47.5%) there was no record of ACV treatment. Hence, where information was available, the majority was immunosuppressed (from treatment for malignancies or infection with human immunodeficiency virus) and not previously treated with ACV. Out of the total number of 130 viable isolates, 66 (50.8%) were found to give the HSV-1 specific product (469 bp size by pol PCR) while 64 (49.2%) gave the HSV-2 specific product (391 bp size). The type-wise ACV susceptibility of the isolates is shown in the table. Of the 130 HSV strains that were tested, 7 (5.4%) were ACV resistant, of which 5 (71.4%) were HSV-2 isolates. The prevalence of ACV resistance among HSV-1 strains was two (3.0%) of the 66 tested. The prevalence of resistance in HSV-2 strains was 5 (7.8%) of 64. The median IC 50 of the HSV-1 strains susceptible to ACV was 0.098 µg/mL (range 0.012-0.39 µg/mL) while that for susceptible HSV-2 was 0.195 µg/mL (range 0.012-0.78 µg/mL). The IC 50 for strains of HSV-1 and HSV-2 resistant to ACV were greater than or equal to 6.25 µg/mL (2 and 5 strains tested respectively). In a previously described study, [4] four isolates were ACV-resistant out of seven clinically resistant HSV-1 isolates tested by plaque reduction assay (PRA). The in vitro method that we used for ACV susceptibility testing was found to be robust and performed reproducibly as assessed by the testing of known standard strains with each batch of tests. Other methods that are described for antiviral testing include the plaque reduction assay (PRA) and DNA hybridization assay (DNAHA). [9] The PRA gives good correlation with clinical response to therapy but requires specialized skill to perform. The DNAHA results in mean IC 50 values that are significantly lower than that from PRA, do not correlate with response to therapy and require the use of radio-labeled probes. We decided to use the DUA even though it has been found to have mean IC 50 values that are about two times greater than for the PRA, since it is simpler to perform and has better discriminating ability in the borderline ACV category. [9] Alternate breakpoints used to define resistance to ACV are 1 µg/mL for HSV-1 and 2 µg/mL for HSV-2. [10] In our study, sensitive isolates had an IC 50 < 1 µg/mL and resistant ones had an IC 50 ≥ 6.25 µg/mL. This finding correlates well with that of other studies that have also shown a bimodal distribution of IC 50 s. [3] In untreated immunocompetent individuals, the mean prevalence of ACV resistant isolates was 0.3% (ranging from 0.1% to 0.7%) while the prevalence in immunosuppressed patients is between 4 and 7%. [3] Of the two patients from whom ACV-resistant HSV-1 isolates were obtained in this study, one patient was immunosuppressed while the status of the other could not be determined. Of the five patients from whom isolates of ACV-resistant HSV-2 were obtained, only one patient was definitely immunosuppressed. There was no definitive record in the case of the other four patients. Discussion The consumption of ACV in our hospital has increased over the years that this study was conducted. Our Pharmacy records show that ACV consumption has increased from 65.5 g per month in 1999 to 101.3 g per month in 2004 for ACV suspension (I.V. preparation), from 3.00 g per month in 2000 to 5.56 g per month in 2004 for ACV eye ointment and from 1.5 g per month to 2.56 g per month in 2004 for ACV cream. However, it has been shown mathematically that HSV drug resistance is predicted to be minimal despite its widespread use (with predictions of only five in 10,000 individuals shedding drug-resistant virus despite high antiviral usage). [11] In summary, the prevalence of resistance to ACV in Indian strains of HSV from this study is 5.4% (7 of 130 strains tested from immunosuppressed as well as immunocompetent individuals). The prevalence of ACV resistance in HSV-1 strains is 3% (2 of 66 tested) and 7.8% (5 of 64) in HSV-2 strains tested. The DU assay is a good screen to determine ACV susceptibility of HSV isolates as it has good reproducibility and is convenient to perform in laboratories in third world countries that have cell culture facilities and an ELISA reader. The prevalence of ACV resistance in these HSV strains is low compared to the increasing usage of ACV in our hospital. This phenomenon will have to be further investigated and seems to be comparable to that from western literature. Acknowledgements The authors thank the Christian Medical College Fluid Research Fund and the Department of Biotechnology, Ministry of Science and Technology, Government of India (BT/PRO658/MDE/09/126/97) for partial financial support. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07072t1.jpg] |
| |||||||||
{kind=link}