 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
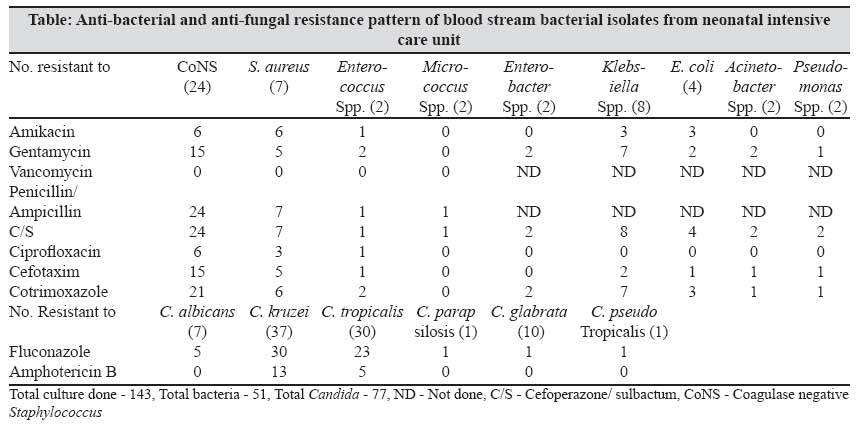
Indian Journal of Medical Microbiology, Vol. 25, No. 3, July-September, 2007, pp. 299-300 Correspondence Etiological and antimicrobial susceptibility profile of nosocomial blood stream infections in neonatal intensive care unit Jain A, Awasthi AK, Kumar M Department of Microbiology, King George's Medical University, Lucknow - 226 001, UP Date of Submission: 06-Feb-2006 Code Number: mb07084 Dear Editor, Nosocomial infections result in considerable morbidity and mortality among neonates, especially in neonatal intensive care units (NICUs). Previous studies have found an incidence of nosocomial blood stream infection (NBSI) in NICUs ranging from 5.2 to 30.4%. [1] The present study was carried out to investigate the etiology of NBSI in NICU and anti-microbial resistance (AMR) of causative organisms. Given the paucity of data from northern India on the profile of bacterial and yeast isolates and prevailing patterns of susceptibility to anti-fungals we speciated 77 (53.8%) yeasts and 51 (35.7%) bacterial isolates obtained between January 2004 and March 2005 from blood culture of neonates and estimated susceptibility to anti-bacterial and anti-fungal drugs. The case inclusion criteria were; hospitalisation in NICU for seven days, intravenous catheter in place and development of clinical sepsis. Exclusion criteria were;> 40 days old, presence of superficial candidiasis and blood culture positive for Candida at the time of admission. Any bacterial or Candida isolate was identified by its colony characteristics, Gram staining, germ tube test, biochemical tests and sugar assimilation and fermentation tests. [2],[3] Antibacterial and anti-fungal susceptibility was performed as per National Committee for Clinical Laboratory (NCCLS) recommendations [4] and disk diffusion method. [5] Details of etiological agents and their anti-microbial susceptibility pattern can be seen in the table. Among 143 hospitalised newborn cases 90 (73.31%) had single, 34 (26.56%) had double and 4 (3.1%) had triple infections. We report a high prevalence of non-C. albicans candidaemia and coagulase negative Staphylococcus septicaemia. High fluconazole resistance along with high resistance to commonly used anti-bacterial antibiotics was also found. Most of the studies have reported high fluconazole and low amphotericin B resistance in Candida isolates. In our NICU, fluconazole is used as the first line anti-fungal agent since last few years. This probably caused a shift towards non- C. albicans resistant strains of Candida spp. Chakrabarti et al . in a five years (1990-1995) report said that isolation rate of non- C. albicans Candida has changed over the years: C. tropicalis (42.1%) and C. guillermondii (15.2%) were common in early 90s, but later there was increase in isolation rate of C. krusei (13%) and C. glabrata (2.2%) (1995). [5] Increased use of fluconazole may have contributed partly to a shift in the incidence of systemic fungaemia due to yeast other than C. albicans which may be less responsive to fluconazole therapy. [6] Nosocomial pathogens have shifted away from easily treatable bacteria towards more resistant bacteria and even to Candida spp. with fewer options for therapy. These shifts continue to present challenges for nosocomial infection control and prevention. References
Copyright 2007 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb07084t1.jpg] |
| |||||||||
{kind=link}