 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
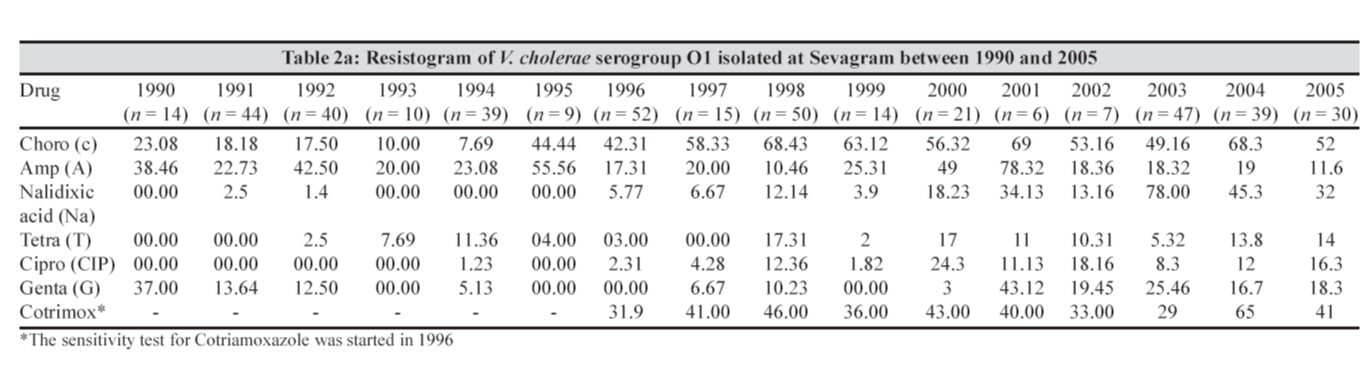
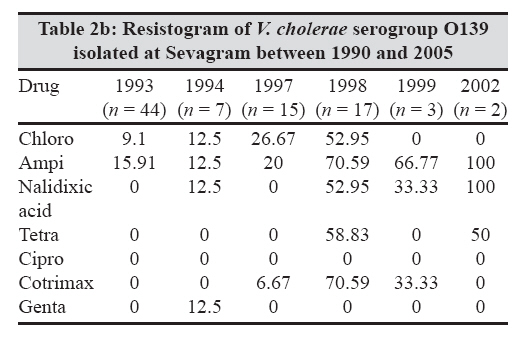
Indian Journal of Medical Microbiology, Vol. 26, No. 1, January-March, 2008, pp. 40-44 Original Article Changing patterns of Vibrio cholerae in sevagram between 1990 and 2005 Narang P, Mendiratta DK, Deotale VS, Narang R Department of Microbiology, Mahatma Gandhi Institute of Medical Sciences, Sevagram, Wardha - 442 102, Maharashtra Date of Submission: 16-Jan-2007 Code Number: mb08008 Abstract Purpose: A retrospective analysis was done to note changes in prevalence, distribution of biotypes, serotypes, antibiotic susceptibility patterns and phage types of Vibrio cholerae isolated in Mahatma Gandhi Institute of Medical Sciences, Sevagram over a period of 16 years. Keywords: Vibrio cholerae, biotypes, antibiotic susceptibility, phage types Cholera continues to be a major concern for the developing countries as it is an important cause of morbidity and mortality. It is an endemic disease with epidemics occurring at regular intervals. Vibrio cholerae O1 El Tor Ogawa has been the offending agent since 1964. However, since 1992, a novel strain - V. cholerae O139 - first isolated in South India, has been responsible for local outbreaks in geographically distinct areas in India. [1] The present retrospective analysis was carried out on the strains of V. cholerae isolated in a rural hospital situated at Sevagram during the last 16 years from 1990 to 2005, in order to determine its prevalence, distribution of biotypes, serotypes, antibiotic susceptibility pattern and phage types. Materials and Methods Mahatma Gandhi Institute of Medical Sciences (MGIMS), Sevagram, is situated in a rural area and caters primarily to the population of Wardha district. A total of 535 strains of V. cholerae were isolated from 10,406 stool and rectal swabs submitted for culture and sensitivity to the Department of Microbiology, MGIMS, from January 1990 to December 2005. The stool samples were collected from patients having signs and symptoms of acute gastroenteritis. Specimens were collected in sterile McCartney bottles before starting antibiotics and transported to the laboratory for processing. The rectal swabs, whenever necessary, were collected with the help of sterile swab sticks and were immediately placed in alkaline peptone water and then transported to the Microbiology laboratory within 2 h. The culture of specimens, identification and biochemical characterization of isolates were done as per standard techniques. [2] Serotyping of the strains was first done in our laboratory by using V. cholerae high titre antisera against O1, Ogawa and Inaba received from C.R.I. Kasauli and O139 obtained from National Institute of Cholera and Enteric Diseases (NICED), Kolkata. All serotypes were confirmed by NICED, Kolkata where the phage typing of the strains was also done by the conventional Basu and Mukherjee phage typing scheme [3] till 1994 and thereafter by the new phage typing scheme. [4] Antibiotic susceptibility testing was performed by modified Stokes Method on Mueller Hinton agar till the year 2000 and there after by Kirby Bauer′s method. The following commercial (Hi Media Laboratories, Mumbai) antibiotic disks were used: chloramphenicol (30 μg), tetracycline (30 μg), ampicillin (10 μg), ciprofloxacin (10 μg), cotrimoxazole (25 μg), nalidixic acid (30 μg), gentamicin (10 μg) and polymyxin B (50 μg). The plates were read after 16-18 hours incubation at 37 °C.The zone of inhibition for each antibiotic was interpreted as per CLSI (previously NCCLS) guidelines. After confirmation, the isolates were stocked in alkaline nutrient agar deeps. The Inaba strains isolated during the year 1999 were further studied for molecular characterization through National Institute of Cholera and Enteric Diseases (NICED) [5] at International Medical Centre of Japan, Shinjuku - ku, Tokyo. Results During the period 1990-2005, a total of 10,406 stool and rectal swabs from diarrhoea cases were processed in our laboratory and 535 (5.14%) V. cholerae were isolated from them. The isolation rate per year ranged from 1.2 to 10.53% [Figure - 1]. Among these, 427 (4.10%) were V. cholerae O1, 86 (0.83%) were O139 and 22 (0.21%) were non O1, non O139. Vibrio cholerae O1 dominated the isolates till 1992 and in 1993 it was almost replaced by O139 [Table - 1]. The O139 appeared in our area in 1993 for the first time and after that it has been periodically isolated. The non O1, non O139 vibrios have also been infrequently isolated from Sevagram. Among O1 vibrios, all the isolates belonged to biotype El Tor. Out of these, 96.01% were of serotype Ogawa. Serotype Inaba was rare till the year 1998 (1990 and 1992 - one isolate each), but became the main serotype in the year 1999, when 11 out of the total 15 (73.33%) V. cholerae isolates were Inaba and reappeared in the year 2005 (4 out of 30 isolates, 13.33%) [Table - 1]. Till the year 1994, phage typing was done by Basu and Mukherjee old phage typing scheme, while from 1995 onwards the new phage typing method was adopted. According to the old phage typing method, 100% clustering of phage types was seen within T2 and T4, while according to the new scheme T27 was the predominant phage type followed by T23, T21, T24, T28 and T20. [Table - 2a and 2b] depict the resistogram of O1 and O139 vibrios, respectively. During the study period, O1 V. cholerae seem to have gained resistance to various antibiotics. However, for tetracycline which is the drug of choice for cholera, O1 isolates were relatively susceptible with maximum resistance recorded being 17.3% in 1998. A very interesting point to highlight here is the resistance to nalidixic acid which had abruptly shown an increase to 78% in the year 2003, while during other years it was between 0 and 45.3%. Resistance to chloramphenicol ranged from 7.69 to 69% during these 16 years. The table also depicts the cotrimoxazole resistance for the year 1996 and onwards when susceptibility testing for this drug was started and resistance ranged from 29 to 65%. The resistance pattern of O139 V. cholerae was different from O1 vibrios. During 6 years (1993-1994, 1997-1999 and 2002) when O139 vibrios were isolated, tetracycline resistance was observed during the years 1998 (58.83% among 17 isolates) and 2002 (one out of two isolates). Ciprofloxacin resistance was not detected in O139 vibrios. The 17 isolates that were recovered during the year 1998 were found to be more resistant as compared to those isolated during other years. Discussion The last decade of the 20 th century witnessed a sharp increase in the global incidence of several emerging and re-emerging infectious diseases. One of the organisms contributing to this global fear of re-emergence was V. cholerae . It reappeared in Latin America in January 1991 after an absence of 100 years in that continent. In 1992, a novel strain V. cholerae O139 Bengal made its presence felt throughout the Indian Peninsula only to disappear after a few years. Such unexplainable explosive outbreaks of V. cholerae continue to occur from time to time making it the most unpredictable organism. More discriminatory procedures and molecular biology techniques are now assisting the epidemiologists in understanding the evolution and spread of V. cholerae clones and emergence of newer variants. However, all these are possible only when the diagnostic laboratories maintain proper records of the detected isolates and endeavour to interpret it in the light of its public health importance. The present article gives a review of the cholera scenario in our area from 1990 to 2005. The important epidemiological tools used were biotyping, serotyping and antibiogram done in MGIMS, Sevagram; phage typing done at NICED, Kolkata; and molecular typing done at International Medical Centre, Japan. During the period under report, average isolation of V. cholerae from all stool samples received was 5.25%, ranging from 1.2% in 2002 to 10.53% in 1994. An outbreak of V. cholerae O139 was reported from our area in 1993 [6] when 44 (81.48%) out of the total 54 cholera isolates in that year belonged to this serotype. The outbreak of the same serotype was also reported from the neighbouring areas of Nagpur and Yeotmal. [1] This serotype was first reported from Chennai in the same year [7] and had spread swiftly throughout the Indian peninsula, virtually replacing the O1 vibrios. It was then speculated that O139 might initiate the eighth pandemic, but fortunately its isolation decreased and since 2003 no O139 vibrio has been isolated in our laboratory. A number of host and environmental factors may be responsible for the diminished isolation of V. cholerae O139. Aquatic environment is the main reservoir for vibrios. [8] One possible explanation put forth is that after the initial period when it caused large epidemics and survived well in the surface water, V. cholerae O139 might have undergone changes; for example, in colonization factors that determine the long-term persistence in the aquatic environment, making the organism less suited for survival. Alternatively, subsequent to the emergence and peak prevalence of V. cholerae O139, V. cholerae O1 might have re-emerged to wipe it out completely and become the predominant organism again. [1] Non O1, non O139 V. cholerae have been known to cause sporadic episodes and small outbreaks of diarrhoea and extraintestinal infections but not epidemics. [9],[10] Non O1, non O139 V. cholerae have also been isolated, though infrequently, in our laboratory. In the year 1998 they were isolated from three children (two of age 9 months and one of age 3 months) with watery diarrhoea and on special request NICED, Kolkata did the serotyping of these strains and they were found to belong to serogroups O6, O23 and O52 (unpublished data). An interesting observation was made with regard to serotypes of V. cholerae O1 in 1999 when 11 of the 15 (73.33%) strains of V. cholerae O1 were Inaba [Table - 1]. Previous to 1999, Ogawa was the prevalent serotype in our area with occasional isolation of Inaba in 1990 and 1992. Such a shift from Ogawa to Inaba was reported from Kolkata in 1989 [9] and from Delhi in 1993 [11] when all the isolates reported were those of serotype Inaba. Periodic shifts in the incidence of Ogawa and Inaba serotypes in a given area is a common phenomenon and is thought to be a consequence of genetic reversal that occurs both in vitro and in vivo . [12],[13] Vibrio cholerae O1 strains of Ogawa and Inaba are known to interconvert particularly in vivo as a result of selection due to immune response during cholera infection. [14],[15],[16] Frequency of conversion from Ogawa to Inaba is fairly common at a rate of 10 -5 and is a result of mutational changes in the gene coding for serotype specificity. [15],[16] A study from NICED, Kolkata has reported that the Inaba strain isolated from different parts of the country in 1998-1999 had probably evolved from the prevailing V. cholerae O1 Ogawa. [5] The Sevagram strains (both Ogawa and Inaba isolated in 1999) were also referred to Kolkata and on the basis of extensive molecular characterization by ribotyping, restriction fragment-length polymorphism and pulse field gel electrophoresis, it was found that these Inaba strains were similar to V. cholerae O1 El tor serotype Ogawa isolated during the same period and were different from the earlier Inaba strains isolated from Kolkata in 1989. [5] In the latest article, NICED has reported isolation of V. cholerae O1 Inaba in 2004 and 2005 from 15 states of India, mostly in the form of outbreaks and have mentioned that the newly emerged isolates were different from the strain earlier prevalent and it was due to mutation in the ′wbeT′gene responsible for serotype conversion. [17] Such information is extremely useful in tracking the source of an outbreak. The study has also shown that the isolates in our laboratory had an increasing tendency to develop resistance to routinely used antibiotics [Table - 2]a and this resistance would emerge in spurts; for example, in the year 2003, nalidixic acid resistance observed was 78%, which was just 13.16% in 2002 and 45.3% in 2004. This pattern of quick shift in resistance is consistent with reports in recent years, which indicate an enhanced mobility in genetic elements like transposons and integrons which confer resistance to antibiotics, [18],[19] making it imperative that all isolates should be subjected to susceptibility testing and resistance patterns should be monitored. Phage typing for V. cholerae is one of the best established tool and marker for epidemiological characterization of the isolates. When old phage typing scheme was used, 100% clustering of phage type was seen within T2 and T4. The new phage typing scheme [4] was found to be more discriminatory with clustering splitting into phage types T27, T23, T21, T24, T28 and T20 in decreasing order. However, some amount of clustering still prevailed and phage type T27, which is the most prevalent type in other parts of India, also remained the prevalent type in our area. The genome of V. cholerae is in a state of constant change, resulting in the emergence of isolates that can either initiate an outbreak or are capable of perpetuating their species in spite of existing high immunity in the community. In the era of rapid transport, there is every possibility of the new strain finding its way into new population and initiating an outbreak. A good data and constant monitoring at least with available tools can help in suspecting and tracing the source of the outbreak. All clinical laboratories, particularly in academic institutes, must endeavour to accumulate the best possible data so that any change, phenotypic or genetic, could be detected at the earliest. The isolates should be religiously sent to the reference laboratories in case the host laboratory is not fully equipped to identify the phage types and the genotypes. Cholera being a notifiable disease, dissemination of information to relevant health authorities and sharing the data with academicians are of utmost importance. Acknowledgement The authors acknowledge the help provided by National Institute of Cholera and Enteric Diseases (NICED), Kolkata for phage typing and provision of O139 antiserum.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08008t2a.jpg] [mb08008f1.jpg] [mb08008t2b.jpg] [mb08008t1.jpg] |
| |||||||||
![[Figure - 1]](/showimage?mb/photo/mb08008f1.jpg){kind=link}
![[Table - 1]](/showimage?mb/photo/mb08008t1.jpg){kind=link}
{kind=link}
{kind=link}
![[Table - 2]](/showimage?mb/photo/mb08008t2.jpg){kind=link}