 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
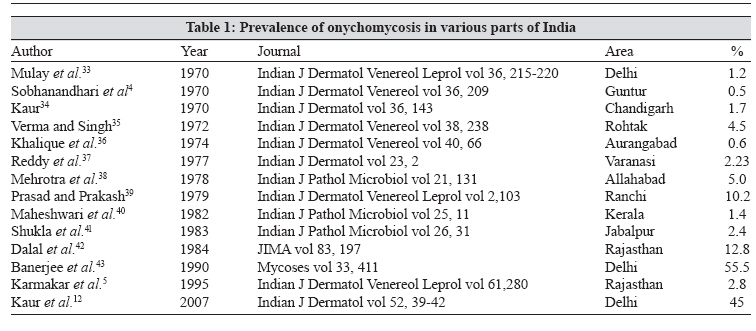
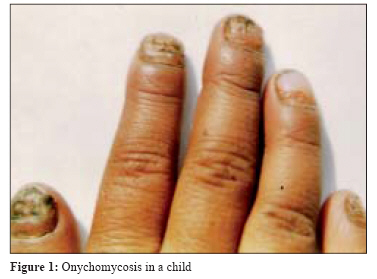
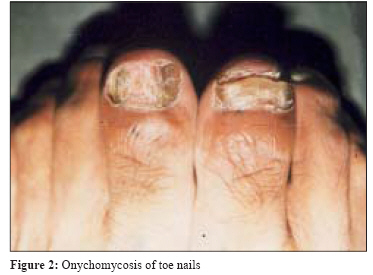
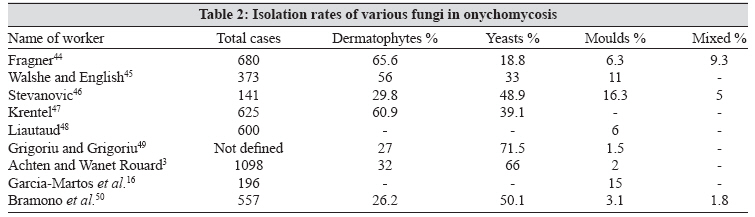
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 108-116 Review Article Onychomycosis - epidemiology, diagnosis and management Kaur R, Kashyap B, Bhalla P Department of Microbiology, Maulana Azad Medical College, Bahadur Shah Zafar Marg, New Delhi - 110 002 Date of Submission: 27-May-2007 Code Number: mb08035 Abstract Onychomycosis is a fungal infection of nails caused by dermatophytes, yeasts or nondermatophyte molds and represents about 30% of mycotic cutaneous infections. Increasingly onychomychosis is being viewed as more than a mere cosmetic problem. In spite of improved personal hygiene and living environment, onychomycosis continues to spread and persist. The prevalence rate of onychomycosis is determined by age, predisposing factor, social class, occupation, climate, living environment and frequency of travel. Onychomycosis in immunocompromised patients can pose a more serious health problem. Dermatophytes are the most frequently implicated causative agents in onychomycosis. Previously regarded as contaminants, yeasts are now increasingly recognised as pathogens in fingernail infections, as are some moulds. Clinical diagnosis of onychomycosis is based on the patients' history; a physical examination, microscopy and culture of nail specimens. The treatment of onychomycosis has been attempted throughout the ages, but only in the last two decades have safe, effective systemic treatments been available for this chronic superficial fungal disease. Oral Griseofulvin and Ketoconazole; once the agents of choice for the treatment of onychomycosis, have been superseded by newer systemic compounds that have a higher cure and lower relapse rates, cause fewer side effects and are suitable for short-term dosing. Keywords: Dermatophytes, diagnosis, nails, onychomycosis, treatment Until the late 1990s onychomycosis was a poorly discussed topic of medical science. Even in financially more advanced Asian countries, onychomycosis has been highlighted only in the last decade. Onychomycosis is a denomination used to describe fungal infection of one or more of the nail units and can be caused by dermatophytes, yeasts or nondermatophyte moulds. [1] Onychomycosis affects approximately 5% of the population worldwide [2] and represents 20-40% of onychopathies and about 30% of mycotic cutaneous infections. [3] Various workers have reported the incidence to vary from 0.5 to 5% in the general population in India. [4],[5] In developing countries, higher priorities in socioeconomic concerns and health issues for other diseases, have resulted in low awareness of onychomycosis by physicians and the general public alike. In spite of improved personal hygiene and living environment, onychomycosis continues to spread and persist. Though there is a clearly diseased appearance associated with this condition, onychomycosis is all too often regarded as merely a cosmetic problem of relatively minor importance that is hardly worth the effort to seek treatment in many cases. This belief may have been supported by the adverse effects and long dosing courses associated with some of the earlier antifungal agents. Only in the last two decades have safe, effective systemic treatment regimens been available for this chronic superficial fungal disease that can have significant negative effects on patients′ emotional, social and occupational functioning. Although onychomycosis is rarely life threatening, its high incidence and prevalence and the associated morbidity makes it an important public health problem. In this paper, current knowledge of the pathogenesis, diagnosis and management of onychomycosis is reviewed. Epidemiology and Risk Factors Reports concerning the prevalence of onychomycosis are conflicting with estimates ranging from 2-3% to 13% in the western population. [6],[7] Unlike in western countries where it is the frequent cause of nail disorders, in Southeast Asia the prevalence of onychomycosis is relatively low. This was partially confirmed by a large scale-survey in Asia in the late 1990s in which the prevalence of onychomycosis was lower in tropical countries (3.8%) than in subtropical countries and the countries in the temperate zone (18%). [8] In India, the prevalence of fungal nail infections has been estimated in the different parts of the country and the observations are listed in [Table - 1]. The prevalence rate of onychomycosis is determined by age, predisposing factor, social class, occupation, climate, living environment and frequency of travel. [9] The prevalence is higher (25%) in patients with human immunodeficiency virus infection (HIV). [10] Several studies have shown that prevalence of onychomycosis increases with age, reasons for which may include poor peripheral circulation, diabetes, repeated nail trauma, longer exposure to pathogenic fungi, sub optimal immune function, inactivity or the inability to cut the toe nails or maintain good foot care. [7] As is the case among adults, prevalence rates for onychomycosis among children are quite variable: a recent review of studies of the subject in several countries lists prevalence rates varying from 0% (United states, Wales and Finland) to 2.6% (Guatemala). The reasons for this 30-fold decrease in the prevalence of onychomycosis in children relative to adults may include reduced exposure to fungus because less time is spent in environments containing pathogens; faster nail growth, smaller nail surface for invasion and lower prevalence of tinea pedis [Figure - 1]. [11] However, the worldwide prevalence of onychomycosis is increasing. In one study that evaluated the prevalence and risk factors of onychomycosis in individuals representing different strata of population in New Delhi the prevalence of onychomycosis was confirmed in 45% of the analysed patients. [12] A number of factors may contribute to this rise. First, as the population ages, there is a corresponding increase in chronic health problems (diabetes) and poor peripheral circulation. Second, the number of persons who are immunocompromised because of infections with human immunodeficiency virus and the use of immunosuppressive therapy, cancer chemotherapy or antibiotics, continue to expand. Third, avid sports participation is increasing the use of health clubs, commercial swimming pools and occlusive foot wears for exercise. [13] In a small percentage of persons, onychomycosis may be caused by a genetic defect that causes an alteration in immune function. [14] Contact with the source of the infection constitutes a risk factor. Other factors that increase the risk of onychomycosis are direct trauma to the nail including nail biting. Onychomycosis in immunocompromised patients can pose a more serious health problem. Not only does the difficult-to-treat infection serve as a constant reminder to the patient of his or her own deteriorated condition, the possibility exists of transfer of fungal pathogens to other individuals. [13]Definition, Etiology and Classification Onychomycosis has been traditionally referred to a non-dermatophytic infection of the nail but is now used as a general term to denote all fungal infections of the nail. Tinea unguium specifically describes a dermatophyte invasion of the nail. The term onychomycosis is derived from the Greek word "onyx", a nail and "mykes" a fungus. Toenails are about 25 times more likely than fingernails to be infected. The longest toe, either the first or the second, which bears the brunt of pressure and trauma from footwear, is particularly susceptible to invasion, although multiple nails are typically infected [Figure - 2]. Dermatophytes are the most frequently implicated causative agents in onychomycosis (nearly 90% in toenail and at least 50% in fingernail infections). Previously regarded as contaminants, yeasts are now increasingly recognized as pathogens in fingernail infections, as are some moulds. [15] The incidence and clinical significance of other than dermatophytic fungi or moulds causing onychomycosis is not well known, because they may be colonising organisms rather than pathogens. The rates of isolation of various fungi in onychomycosis are listed in [Table - 2]. One report, which presented the results of a two-year study, conducted to determine the incidence and aetiology of onychomycosis by nondermatophytic fungi in the population of Spain, described a number of species, such as Fusarium spp., Scytalidium spp. and Acremonium spp. etc. as aetiological agents of onychomycosis. [16] Nondermatophyte moulds cause 1.5-6% of onychomycosis. [17] Onychomycosis secondary to nondermatophyte moulds is seen most frequently in the elderly, in patients with skin diseases that affect the nails and in immunocompromised patients. It is more frequent in toes than in fingers. Many of these fungi are highly sensitive to cycloheximide and may be missed if the specimen is not also inoculated on a cycloheximide-free medium, such as Sabouraud glucose agar, Littman′s Oxgall agar or potato dextrose agar. Clinical clues that a nondermatophyte mould is the causative pathogen may include the absence of tinea pedis, only one or two infected toenails, a history of trauma, a history of nonresponsiveness to systemic antimycotics and association with periungual inflammation. There are three groups of fungi associated with onychomycosis: dermatophytes, non-dermatophytic moulds and yeasts. Common Fungal Agents Associated with Onychomycosis
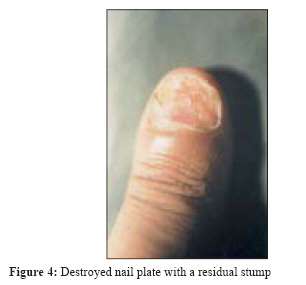
Clinical Presentation and Patterns of Fungal Invasion in Onychomycosis Distal subungual onychomycosis Proximal subungual onychomycosis White superficial onychomycosis Candida onychomycosis Candida paronychia: This is the most common type and is marked by swelling and erythema of the proximal and lateral nail folds, also called a "whitlow". After infection of the nail matrix occurs, transverse depressions (Beau′s lines) may appear in the nail plate, which becomes convex, irregular and rough and ultimately dystrophic. Candida granuloma: This type is uncommon and is characterised by direct invasion and thickening of the nail plate and associated paronychia. This condition is seen in immunocompromised patients. The organism may affect the entire thickness of the nail, resulting in advanced cases, in swelling of the proximal and lateral nail folds until the digit develops a pseudo clubbing or "chicken drumstick" appearance. It is useful to take sample from both the nail plates as well as the subungual debris of the infected nail. Candida onycholysis: This occurs when the nail plate separates from the nail bed. Distal subungual hyperkeratosis can be seen as a yellowish grey mass lifting off the nail plate. The lesion resembles that seen in patients with DSO. Total dystrophic onychomycosis (TDO) : In this type there is total destruction of the nail plate, which usually may be the end result of the any of the four main patterns of onychomycosis. The entire nail unit becomes thick and dystrophic. TDO is used to describe end-stage nail disease, although some clinicians consider it a distinct subtype [Figure - 4]. Diagnosis of Onychomycosis Increasingly onychomychosis is being viewed as more than a mere cosmetic problem. Persons with unsightly infected nails may suffer embarrassment. Fungi from the nails may precipitate secondary bacterial infections, cellulitis, idiopathic reactions and chronic urticaria. Infected toenails may act as a reservoir for fungi, facilitating their transmission to other areas of the body and may even to other people. Clinical diagnosis of onychomycosis is based on the patients′ history; a physical examination, microscopy and culture of nail specimens. Predisposing factors like diabetes, old age, hyperhydrosis, onychoglyphores, nail trauma, poor peripheral circulation are likely to be present. Several nail disorders that may mimic fungal nail infections must be differentiated from one another and onychomycosis to initiate the most appropriate therapy. They include psoriasis, lichen planus, bacterial infections, contact dermatitis, traumatic onychodystrophies, paronychia congenital, nail bed tumours, yellow-nail syndrome, idiopathic onycholysis etc. One should look for cutaneous signs of psoriasis on the scalp, gluteal folds, elbows and knees and nails should be evaluated for other signs of psoriasis, especially for pitting and/or small salmon coloured droplets evident on the plate. Approximately 10% of patients with lichen planus have abnormal nails. [2],[4] A practitioner can differentiate lichen planus by looking for the violaceous purple papules ridged/dystrophic nail indicative of lichen planus on the extremities or by other signs on the mucus membranes. Repeated nail trauma can cause distal onycholysis, leading to colonization of the affected space by microorganisms that produce pigmentation of the area. If the onycholytic nail is clipped to allow examination of the nail bed, the latter will be normal if the symptoms are caused by trauma rather than onychomycosis. A habit tic, often manifestating as a median furrow or depression in the middle of the nail, may also cause abnormalities of the nail. The yellow nail syndrome may also be mistaken for a fungal infection; however, the hardness of the nail plate, its increased longitudinal curvature and the light green/yellow discoloration are all typical and discriminatory. Specimen collection For distal subungual onychomycosis, the abnormal nail is clipped proximally and the nail bed and underside of the nail plate are scraped with a 1-2 mm serrated curette; the outermost debris should be discarded. Care should be taken to avoid penetration of the nail plate and bleeding. It is important to obtain nail material from the advancing infected edge closest to the cuticle, where the likelihood of viable hyphae is the greatest. For proximal subungual onychomycosis, the normal surface of the nail plate is pared down with a no. 15 surgical blade at the lunula and the white debris is collected with a sharp curette from the deeper portion of the plate and the proximal nail bed. For WSO, the white spots on the nail are scraped and the outermost surface is discarded; the white debris directly underneath is then collected. For Candida infection, the material closest to the proximal and lateral nail edges should be obtained. If Candida onycholysis is suspected, the lifted nail bed and, if necessary, the under surface of the nail plate are scraped. For TDO, any abnormal area of the nail plate or bed can be used as a specimen. The sampled material can be divided into two portions: one for direct microscopy and the remainder for culture. If nail material is to be used, fine shavings or minute clippings are preferred to large pieces. The specimen should be obtained when the patient has been off both topical and systemic antifungal drugs for two to four weeks. If the specimen is shipped to an outside laboratory, a sterile container, a pill packet, a clean sheet of white paper folded and sealed with tape or a specially designed mailer such as a Dermapak TM can be used. Specimens must not be kept in moist media to avoid rapid multiplication of bacterial and fungal spores. Ideally nail specimens should be processed within a week, although infective fungal elements can remain viable for months after specimen collection. Specimen analysis Two different media are used for culturing nail specimens; primary medium (containing cycloheximide selective against most nondermatophytic molds and bacteria) such as dermatophyte test media (DTM), Mycosel (BBL) and Mycobiotic (DIFCO) and secondary medium (free of cycloheximide that allows isolation of nondermatophytes nail pathogens) such as Sabouraud glucose agar, Littman′s oxgall medium and potato dextrose agar. The addition of antibiotics such as chloramphenicol and gentamicin to Sabouraud glucose agar or potato dextrose agar is an additional precaution to eliminate bacterial contamination from non-sterile sites. Ideally the specimen should be incubated at 25-30°C. The incidence and clinical significance of other than dermatophytic fungi or moulds causing onychomycosis is unknown, because they may be colonising organisms rather than pathogens. Therefore, reference laboratories should provide data on whether the isolated fungus was a likely pathogen or an unlikely one. All dermatophytes should be considered pathogens. To increase the predictive power of a diagnosis of dermatophytic invasion of a nail, Summerbell [21] suggested that non-filamentous non-dermatophytes identified in nail tissue may be considered as one of the following:
As an additional confirmatory technique, definitive identification of non-dermatophytic invasion in nails may require the isolation of the agent from successive specimens from the infected region. The difficulty in isolating fungi from nail clippings in cases of onychomycosis because of the non-viability of the fungal hyphae in the distal portion of the nail plate from where the scraping is done is well known. In order to improve the isolation rate various methods have been derived. These include the use of a grinder [22] or a dental drill fitted with a suction nozzle, [23] which collects the nail dust for microscopy and culture. This latter instrument has raised the success rate of culture from microscopically positive nails from the usual reported rates of 50-75% to about 88%, but is not a practical procedure for the routine laboratory. [24] If neither microscopy nor culture yields a diagnosis, histological analysis of pulverized nail plate clippings will determine whether the pathogen is a fungus. This procedure is helpful when the patient has a dystrophic nail that has repeatedly failed to show a positive response with potassium hydroxide or culture. Nail plate fragment can be sent in a 10% buffered formalin container for histopathologic analysis such as periodic acid-Schiff (PAS) staining. PAS stains glycogen and mucoproteins in the fungal cell wall. In one recent study, PAS was found to be more sensitive than KOH preparation and culture alone (92% versus 80% or 59% respectively) and PAS staining plus culture had the best sensitivity overall. [25] Another advantage of histopathologic evaluation with PAS is the short time required to render a diagnosis compared to culture. Histopathology reliably demonstrates whether a fungus is invasive or merely colonising subungual debris but like KOH this preparation does not identify the particular pathogen. PAS stain is usually sufficient to demonstrate fungi; however, small serum inclusions may be mistaken for fungi, as they are also PAS positive. The methenamine silver stain (Grocott) and calcofluor white are more selective. Nail biopsy is the last resort. Treatment of Onychomycosis As can be imagined, the treatment of onychomycosis has been attempted throughout the ages, but success has been limited until the current decade. In choosing therapy, the physician needs to consider the patient′s age and health, the infecting organism, potential side effects and drug interactions of the various agents, the cost of treatment, the dosage schedule and patient compliance. As the rate of growth of toenails is one-third to one-half of fingernails, therapy of the former using the classical systemic drugs such as griseofulvin and ketoconazole must be continued for 12-18 months whereas fingernail infections may be cured in six months. Oral griseofulvin and ketoconazole; once the agents of choice for the treatment of onychomycosis, have been superseded by newer systemic compounds that have a higher cure and lower relapse rates, cause fewer side effects and are suitable for short-term dosing. [26] Griseofulvin represented a promising advance in antifungal therapy when it first became available for clinical use nearly forty years ago. However, its effectiveness proved a disappointment, since its spectrum of activity is limited to dermatophytes and a prolonged duration of therapy is required for maximal efficacy-a period that may last for more than one year. Poor compliance with long-term therapy as a result of the side effects and the slow and incomplete clearance of dystrophic nails, led to success rates as low as 3-38%, with recurrence of infection often observed. [27] Ketoconazole, developed in the 1980s, was the first orally active imidazole with a relatively broad spectrum of activity against dermatophytes, some yeast and several moulds. However, the long-term use of oral ketoconazole in onychomycosis, which is necessary to effect improvement or cure, is limited by the occurrence of side effects and significant drug interractions. [28] The newer antifungal agents (itraconazole, fluconazole, terbenafine) block the ergosterol synthesis pathway at different points, a difference with implications for these drugs′ efficacy and side effects. Fluconazole, a triazole developed in the 1990s, is active against dermatophytes, Candida spp. and certain other fungi. Studies of fluconazole in onychomycosis show high cure rates but a need of long treatment time along with demonstration of some potentially significant drug interactions. [29] Itraconazole, a broad-spectrum synthetic antifungal triazole approved in 1995 for the treatment of onychomycosis, represents an advancement beyond earlier therapies, due to its broad spectrum of activity, its high affinity for keratin and its pharmacokinetic profile. It is highly effective in the treatment of dermatophyte, yeast and some non-dermatophytic mould infections of the nails. Due to its rapid penetration into the nail and prolonged presence in the nail after discontinuation of drugs; Itraconazole has been evaluated in intermittent dosing or "pulse therapy" regimes which consists of dosing for one week (pulse) per month for a set number of months. [30] The allylamine antifungal agent terbenafine is effective against dermatophytes and some moulds but has less activity in C. albicans infections. Results from several studies show that terbenafine has a high mycological cure rate and it significantly reduces treatment time over the older systemic agents. [31] Regardless of which continuous oral antifungal agents the physician prescribes, a baseline liver profile and a blood chemistry study are recommended; however, this is not indicated for itraconazole pulse therapy. Topical antifungal agents are of limited efficacy when used alone or with older antifungal agents to treat onychomycosis, but they may result in a more rapid cure when used in conjunction with the newer systemic compounds. They may also help to prevent the recurrence of tinea pedis, which often accompanies fungal toenail infections. Topical therapy has the greatest potential as primary therapy in mild infections, as palliative therapy in those unable to take oral therapy and as a prophylactic agent. Improvement of the conventional formulations led to the development of an alcoholic solution containing 28% tioconazole and undecylenic acid, for instance, which has produced moderate results. [32] A further step forward has been achieved with the development of new vehicles in the form of colourless nail lacquers known from cosmetic formulations. Two compounds, amorolfine and ciclopirox, are currently used in a lacquer base in several countries. Surgical nail removal is not often used because of the discomfort, cost and possible cosmetic disfigurement. Avulsion of the nail combined with a topical antifungal agent, under occlusion, may be effective in selected patients. However, because of the inherent problems of nail avulsion, this is best limited to those with only one or two dystrophic nails and those intolerant of oral antifungals. Total surgical removal has to be discouraged: the distal nail bed may shrink and become dislocated dorsally. In addition, the loss of counter pressure produced by the removal of the nail plate allows expansion of the distal soft tissue and the distal edge of the regrowing nail then embeds itself. This can be largely overcome by using partial nail avulsion. Chemical avulsion, done by urea ointment, is a painless method that has superseded partial surgical avulsion. Preventing recurrence and relapse Following are some suggested measures:
References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08035f4.jpg] [mb08035f3.jpg] [mb08035f1.jpg] [mb08035t2.jpg] [mb08035t1.jpg] [mb08035f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}