 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
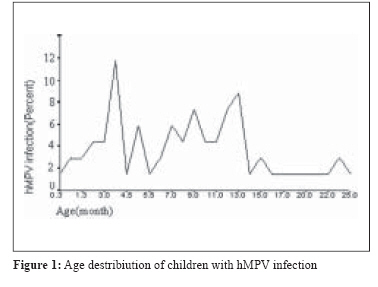
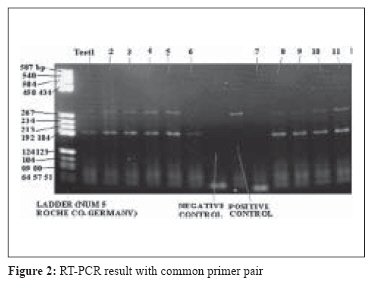
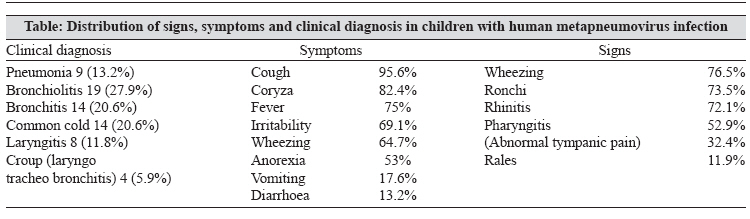
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 123-126 Original Article The highest prevalence of human metapneumovirus in Ahwaz children accompanied by acute respiratory infections Arabpour M, Samarbafzadeh AR, Makvandi M, Shamsizadeh A, Percivalle E, Englud Janet, Latifi Seid Mannut Division of Virology, Department of Microbiology-Faculty of Medicine - Ahwaz Jondishapur University of Medical Sciences, Ahvaz Date of Submission: 07-Jun-2007 Code Number: mb08037 Abstract Purpose: The newly described human metapneumovirus (hMPV) has been recently discovered as an etiological agent of acute respiratory infections (ARTI) in infants and children. The aim of this study was to determine the prevalence of hMPV and its potential role as causative agent of ARTI in Ahwaz children.Methods: In the present study, we examined 124 nasal swabs from infants affected by ARTI for the presence of hMPV by RT-PCR technique. Results: Sixty-eight out of 124 (54.4%) cases were positive for hMPV which is the highest incidence of hMPV ever reported in the world, 94.1% of positive cases belonged to genotype A; whereas no B genotype was detected. Our positive hMPV children were affected by upper (URTI) as well as lower respiratory tract infection (LRTI); however, LARTIs had higher prevalence. Conclusions: We suggest a probable role of F protein alteration as the causative agent for the highest prevalence of hMPV infection among Ahvaz children. Keywords: Ahwaz, acute respiratory infections, human metapneumovirus Human metapneumovirus (hMPV), a new human respiratory virus pathogen belonging to genus Metapneumovirus (family Paramyxoviridae, subfamily Paramyxovirinae), has been recently discovered in 2001 by Dr. Van Den Hogen, in nasopharyngeal aspirates from children affected by ARTI. [1] Two distinct genotypes have been described called type A and B, with a variable prevalence in the world. [2],[3],[4],[5],[6] hMPV has been shown to be responsible for a significant portion of ARTI in early infancy and childhood as well as in the elderly and immunocompromised host. [1],[3],[6],[7] hMPV is the second virus after human respiratory syncytial virus (hRSV) with the highest prevalence of ARTI (43%) among children and infants. [2],[3],[4],[7],[8] In the present study, we investigated the virological and clinical features of hMPV in children. Materials and Methods During 2005 fall/winter seasons, nasal discharge samples from 124 children below two years of age and affected by ARTI, were collected using dacron swabs. Each swab was swashed in a microtube containing 200 μl phosphate buffer solution (PBS). Samples were finally stored at −70°C until usage according to previous instructions. [8] All samples were thawed at 25°C and viral RNA was extracted with Roche pure viral nucleic acid kit and converted to cDNA by using Qiagen Sensiscript Reverse Transcriptase. The samples were then screened for hMPVby carrying out a PCR reaction with the common pair primer targeted regions of hMPV F gene that was conserved among Dutch, Australian, and Connecticut strains. [9] The forward primers, 5-GCGCGTTCTGAGGACAGGTTGG and reverse primers, 5-GCGCTCAAGCCGGA TGGTTTTGG, produced an amplicon that corresponds to nt 111-392 of the hMPV F gene (GenBank accession number AF371367). Concentrations of PCR reagents were as follows: 0.5 μm, MgCL2 1.5 mm, dNTP Mix 0.2 mm, Taq polymerase 1.25 U. The first reaction was performance at 95°C for 15 minutes; then 35 cycles for 1 minute. 94°C, 45-55°C for 1 minute, 72°C for 1 minute; 72°C for 10 minutes as previously described. [9] Negative samples for common primers were checked for the accurate performance of extraction and RT steps by carrying out a PCR reaction on RT products for 18s rRNA as previously described. [10] hMPV typing on positive samples was performed with two separate set of primers. For type A, a 170-bp segment of the L gene spanning nucleotides from 11321 to 11490 of hMPV prototype strain 00-1 was amplified by antisense primer (5-CACCCCAGTC TTTCTTGAAA-3; positions 11471 to 11490) and sense primer (5-CATGCCCAC TATAAAA GGTCAG-3; positions 11321 to 11342) under previously described conditions. [11] For type B, a 169 bp segment of the L gene spanning nucleotides from 4121 to 4290 covered both genotype B1 and B2 was amplified by forward primer: 5-TATGCCTACTATAAAA GGTCAA-3; Reverse Primer: 5-CACCCCAGTCTTTCCTAAAG-3-under previously described conditions. [5] Finally, to rule out the presence of hRSV, the most frequent respiratory viral agent responsible for ARTI, a nested RT-PCR was carried out on hMPV positive samples as previously described. [12] Results hMPV prevalence among male (48.5%) and female (51.5%) patients was almost similar. A further analysis by two-tailed independent T test showed that there was no correlation ( P -value > 0.05) between gender in children less than two years and the rate of infection due to hMPV. The age of hMPV positive children was between 10 days and 24 months and the average age was 17 months. Age distribution of hMPV positive children is reported in [Figure - 1]. Sixty eight out of 124 (54.4%) samples were positive for Hmpv. Among positive samples 94.1% belonged to Genotype A [Figure - 2], whereas no genotype B was detected; 5.9% of positive cases remained untypable. 33.8% (23/68) of hMPV positive children were co-infected by hRSV. An interesting observation in PCR results with hMPV common primer was that an extra band of 192-184 bp could be observed beside the main band of 281 bp, but not in positive control which was obtained from an Italian isolate. The extra band could not be eliminated modifying the PCR conditions such as lowering the MgCl 2 solution concentration and/or increasing the annealing temperature [Figure - 2]. To ensure that this extra band was not a chromosomal spurious band we made an extra experiment with whole blood extracted nucleic acid as template and no extra band was detected. A comparative correlation of hMPV infection frequency with clinical manifestation in ARTI is reported in the table. Statistical analysis did not demonstrate any significant correlation between each clinical manifestation and the positivity for hMPV: χ2 test P -value = 0.140. Further analysis showed a significant difference between the rate of hMPV infection in LRTI (pneumonia, bronchiolitis and bronchitis) versus URTI in favor of LRTI. Signs and Symptoms associated with the presence of hMPV are reported in the table. Seventy-four percent (50/68) of positive cases were less than 12 months old. Statistical analysis showed that there was no significant linear correlation (Pearson Correlation test P -value = 0.065) between an increase in age and hMPV infection rate; although the rate of hMPV infection showed a strong correlation in the 0-12 months age group (χ2 P -value < 0.001), versus the 12-24 months age group. HMPV infection rate was 54.2% in fall and 56.4% in winter, with almost no statistical difference. In addition, our analysis revealed no significant correlations between the rate of infection and meteorological indices: amount of precipitation ( P = 0.5) number of days with thunder storm or dust ( P > 0.6), air temperature ( P = 0.508), air pressure ( P = 0.795) and relative humidity ( P = 0.64). Discussion As previously described, the prevalence of hMPV in children population is between 1.5 and 43%, but the prevalence of hMPV among Ahwaz children was the highest so far reported in the world (54.2-56.4%). [2],[3],[4],[5],[8],[12],[13] According to other reports, [5] our results confirmed that wheezing and cough were in order the most prevalent sign and symptom in hMPV positive children affected by ARTI [Table - 1]. In addition, our study showed that bronchiolitis was the most significant clinical diagnosis associated with the presence of hMPV: 28% compared to 67% reported in other studies. [4] Despite the fact that in our study hMPV cover a broad rang of URTI and LRTI, we found that hMPV was involved in LTRI rather than UTRI. [2],[3],[4],[5],[8],[12] The rate of hMPV infected children was inversely proportional to their age: a decrease in rate of infection was associated with an increase in age. This finding is in concordance with the fact that by the age of five months almost all of the children had encountered hMPV. [12] The reasons for high prevalence of hMPV among Ahwaz children could be either viral internal factors like the efficiency of viral replication, the ability of the virus to escape from host immune responses, the route of transmission or environmental factors that are not totally independent from the former factors and include geographical position, climate situation, seasonal fluctuation, yearly variation and finally genetic susceptibility of patients. [2],[13] Moreover, in a definite geographical region, factors like the patient age, their health, the rate of circulating antibodies and the genetic characteristic of the population can be determinant factors. Previous studies have shown that there are three major surface antigenic determinants in hMPV called G, SH and F glycoproteins. [1],[2] Although hMPV G and SH glycoproteins are the most capable for the genetic heterogeneity of hMPV, only immunity against F protein is considered to be significantly neutralizing or protective. [14] Further studies have shown that some alteration in the F gene, may confer a host immunological evasion to the virus without having an interaction with viral growth or virulence. [15] As earlier mentioned, the result of RT-PCR experiments in this study with the hMPV common pair primers resulted in an extra band which is equal to an extra recognition site inside the F gene. Since an extra recognition site could not be created unless a sequence alteration carried out, this phenomenon raises the hypothesis that an alteration that happens in F gene led to a genetic heterogeneity accounting for host immune evasion. However, further investigations are needed to prove this hypothesis. Another hypothesis for the probable role of immune evasion in high prevalance of hMPV in Ahwaz could be the age of the children involved. It has been shown in previous studies throughout the world that children less than six months had fewer infections than children between 6 and 12 months. [2],[3],[4],[5],[13] In our study the age of infection was under six months and also in children belonging to the two groups of 0-6 months and 6-12 months the infection rate was the same. Since it is generally believed that maternal immunity is capable of conferring immunity against most of infectious agents in babies less than six months, a decrease in infection age could be an indication that maternal immunity did not work well against a potential new variant of hMPV. As mentioned before, the geographical distribution of hMPV infection in children less than 6 months is variable through out the world. Because Ahwaz climate is similar to a tropical region it is comparable with a South American country like Brazil (17%) even if Ahwaz is situated in the northern hemisphere. [2] HMPV prevalence in Ahwaz is three times higher than in Brazil. On the other hand our data are very close to that reported from Italy (43%). [8] So the climate contribution in the prevalence of hMPV might not be the major factor influencing the high prevalence of this virus in Ahwaz city. Yearly genetic variation may be responsible for viral evasion from pre-existing immune response due to the circulation of another genotype. [8] Since we carried out our experiment during one year we could not estimate the effect of the above factor on hMPV prevalence. Many studies have confirmed the role of seasonal fluctuation in hMPV prevalence. [2] As previously mentioned, no significant difference was observed between fall and winter in hMPV prevalence in this study. Another factor that may contribute to the high hMPV incidence is the genetic susceptibility of the population. Although no studies have yet analysed the effect of this factor on the prevalence of hMPV, some previous studies revealed the influence of genetic susceptibility on the incidence of other human paramyxovirus infections. [16] Since we did not rule out all of respiratory viral agents in our hMPV positive children we can not conclude that hMPV was the sole causative agent of all ARTI in this study. However, our results showed that RSV, which has been confirmed to be the major causative agent of ARTI in children less than five years, coinfected only 1/3 of our hMPV positive cases. This data raises the probable role of hMPV as an important causative agent of ARTI. Considering all the factors that may contribute to the high prevalence of hMPV infection among Ahwaz children, we suggest a role of F protein alteration as the most probable causative agent. Acknowledgements The authors thank Janet Englud (Regional Medical Center, Seattle, USA), Zohre Younesee (Abouzar Hospital, Ahvaz, Iran) and Seid mahmoud Latifi (Statistic departments, Ahwaz Jondishapur University, Ahvaz, Iran) for helping with this study.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08037t1.jpg] [mb08037f2.jpg] [mb08037f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}