
|
Indian Journal of Medical Microbiology
Medknow Publications on behalf of Indian Association of Medical Microbiology
ISSN: 0255-0857 EISSN: 1998-3646
Vol. 26, Num. 2, 2008, pp. 127-131
|
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 127-131
Original Article
Advantage of using a home-made elisa kit for detection of Helicobacter pylori infection over commercially imported kits
Mohammadi M, Talebkhan Y, Khalili G, Mahboudi F, Massarrat S, Zamaninia L, Oghalaei A
Biotechnology Research Center, Pasteur Institute of Iran
Correspondence Address:Biotechnology Research Center, Pasteur Institute of Iran
marjan@pasteur.ac.ir
Date of Submission: 10-Aug-2007
Date of Acceptance: 27-Sep-2007
Code Number: mb08038
Abstract
Purpose: To evaluate a home-made ELISA kit for detection of Helicobacter pylori (Hp) infection and comparison of its immunologic criteria with those of foreign commercial kits.
Methods: A home-made IgG ELISA kit was developed using soluble antigenic fractions of Hp proteins. Confirmed sera were tested and serological criteria were evaluated through assessment of 199 serum samples.
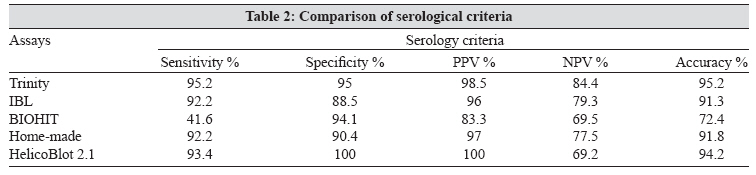
Results: The accuracy, sensitivity and specificity values of home-made kit were 92, 92 and 90.4%, respectively. These immunologic criteria for Trinity kit were 95.2, 95.2 and 95% in comparison with IBL kit (91.3, 92.2 and 88.5%), BIOHIT kit (72.4, 41.6 and 94.1%) and HelicoBlot2.1 (94.2, 93.4 and 100%). Kappa agreement assessment demonstrated that two of the imported ELISA kits had fair to moderate agreement with the home-made kit while the other one had a poor agreement value.
Conclusions: Apart from comparable values between the home-made kit and the most efficient imported kit (Trinity) there was significant cost benefit. Therefore, we recommend the home-made kit as a suitable substitution for detection of Hp infection in the Iranian population.
Keywords: Helicobacter pylori, IgG ELISA, serology, screening
Helicobacter pylori (Hp), a gram negative bacterium, infects the gastric mucosa in humans and induces several gastrointestinal complications ranging from mild gastritis (asymptomatic) to peptic ulcers and even gastric malignancies, [1] such that the International Agency for Research on Cancer (IARC), has declared this pathogen as an independent carcinogen. [2],[3] In addition, the etiologic association of this infection with an increasing number of disorders, including cardiovascular diseases, [4] skin allergies and autoimmune diseases are further revealed. [5] The incidence of Hp infection in the developed countries ranges from 30 to 50% of the population [6] whereas that of developing countries such as Iran reaches 60-90% of the general population. [7],[8],[9] Since Hp infection, in addition to causing problematic symptoms, may lead to gastrointestinal ulcers and gastric malignancies, it is of utmost essence to detect the infection at early stages and pursue with eradication therapy and follow-ups.
Currently the most indicative and precise method of diagnosis is endoscopy followed by colorimetric enzyme assays as the gold standard tests for the diagnosis of Hp infection. However, only those experiencing intolerable symptoms with indications of progressive disease are referred for endoscopy. The rest of the population remains undetected and untreated. On the other hand, the invasive method of endoscopy is quite unappealing and is met by severe hesitations. A simple cost-effective diagnostic procedure which would bypass the need for endoscopy is highly required for a population like Iran in which the rate of infection is overwhelming. Inclusion of a reliable diagnostic test into the routine medical check-ups will provide secure means for controlling the population health and devising appropriate preventive and therapeutic regimens.
Serological detection of Hp infection is one of the major non-invasive methods which can be used in epidemiological studies, enabling us to screen patients suffering from dyspepsia before performance of endoscopies and for long term follow-ups subsequent to drug therapy. Despite the fact that serum levels of IgG and IgA against Hp surface antigens drop within 2-6 months following treatment, they do not return to their initial titres before acquisition of infection. [10] Collectively using serological tests, especially for infants, children and disabled individuals; is preferable over invasive techniques such as endoscopy and biopsy sampling.
The most frequently used serological test for Hp detection is ELISA due to its simplicity, low cost and high sensitivity. There are several ELISA tests developed in different countries which can be used in the diagnosis of infection. Commercial serological assays for Hp detection demonstrate varying accuracies for different populations which may be due to the vast molecular diversity in genes and encoded proteins among isolated Hp strains from different geographic regions used for the coating antigen preparations. [11],[12]
In this study a home-made ELISA kit was developed incorporating soluble antigens extracted from Iranian Hp strains and evaluated against commercially used imported ELISA kits.
Materials and Methods
Subjects
A total of 199 subjects including 180 dyspeptic patients who referred to three major hospitals for endoscopy and 19 asymptomatic volunteers were included in this study after obtaining informed consent. The asymptomatic individuals were included for confirmation of true negative subjects. Cases were considered and included as Hp-positive if (1) bacterial culture or (2) rapid urease test (RUT) and histology were found positive. Hp negative cases were included as those with no Hp-positive test results and were additionally confirmed as negative by urea broth test (UBT). Patients under medications such as antibiotics, antacids and H2 blockers for a period less than four weeks prior to endoscopy were excluded from this study.
Sampling
At endoscopy, biopsy sampling was performed after obtaining informed consent. Gold standard diagnostic tests were based on sampling three antral biopsy specimens followed by RUT, bacterial culture and histology. For RUT, one biopsy specimen was immediately placed into 0.5 mL urea indicator broth at room temperature. Any change in colour from yellow-orange to pink in the next two hours indicated the presence of Hp in the sample. Homogenized gastric biopsies were cultured on brucella agar plates supplemented with 5% sheep blood. Plates were incubated at 37°C under microaerophilic conditions for 5-7 days. The grown bacteria were identified as Hp via microbiological and biochemical tests. Histology slides were Giemsa stained and scored for the presence of Hp in several fields. 13 C-urea breath test (with adjusted cut-off values for the Iranian population) was also used to confirm Hp negative subjects. One breath sample was collected after drinking 13 C-urea solution. Five millilitres of venous blood was also obtained from every subject for serological studies. Serum samples were collected and stored at −20°C for serological tests.
Soluble antigenic fraction of H. pylori
A cocktail of Hp strains isolated from subjects with various clinical pictures (NUD, PUD and GC) was prepared. Genotyping studies on two Hp virulence markers ( cagA and vacA genes) were performed indicating that the above cocktail was composed of all possible genotypes of the above mentioned genes ( cagA+/− and s1m1, s1m2, s2m2 genotypes of vacA ). The bacterial pellet was weighed and resuspended in PBS (0.3 g/mL). The suspension was incubated on ice for 1 h. Sonication was performed on ice for 15 x 45 s pulses with equivalent intervals in order to confirm disruption of all bacterial cells. The sonicated solution was centrifuged at 11,000 g for 30 minutes. The supernatant was then transferred to a new tube and passed sequentially through 0.8, 0.45 and 0.22 μm filters. This solution, which contained the entire Hp soluble antigens was electrophoresed and analysed on a 15% SDS-PAGE and was used as coating antigen in ELISA.
Initial standardisation
MaxiSorp 96 microtiter plates (Nunc, GmbH, Germany) were coated with 100 μl of varying concentrations of cocktail Hp soluble fractions 0-50 μg/mL prepared in carbonate bicarbonate buffer (pH 9.6) and incubated overnight at 4°C. The coated wells were blocked with phosphate buffered saline (PBS) containing 1% bovine serum albumin (BSA, Sigma) for two hours at room temperature (RT). Confirmed Hp positive and negative sera (based on the gold standards) were used for standardisation of the assay. These sera were diluted 1:100 in PBS containing 1% BSA and 0.1% Tween-20. Microtiter wells were incubated for one hour at RT. Plates were then washed five times with PBS-Tween. Wells were incubated with serial dilutions (1:5000-1:100,000) of the secondary antibody, HRP conjugated polyclonal rabbit anti human IgG (DAKO, Denmark), for one hour at RT. Plates were then washed and incubated with tetramethylbenzidine (TMB), as the substrate, for 10 minutes at RT. Optical densities (OD) were measured for duplicate serum samples at 450 nm using a standard 96-well microtiter plate ELISA spectrophotometer (BIOHIT, Finland). The appropriate antibody dilution was determined using serial dilutions ranging from 1:100 to 1:1000 while keeping the concentration of coating antigen and secondary antibody constant.
Validation and determination of cut off value
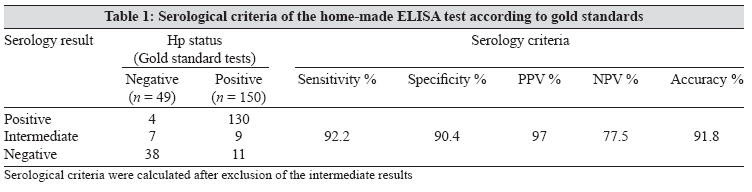
Endoscopy based gold standard tests including RUT, Hp culture and histology were used to categorise subjects into 150 Hp-positive and 49 Hp-negative cases. Home-made ELISA kit was validated using these Hp-positive and negative sera and the serology criteria were calculated according to their standard definitions.
Evaluation of home made ELISA kit against commercially imported kits
Home made ELISA kit was compared with three commercially available ELISA kits including Trinity (Trinity Biotech PLC, Bray, Ireland), IBL (IBL Immuno Biological Laboratories, Hamburg, Germany), BIOHIT (BIOHIT PLC, Helsinki, Finland) and one western blotting kit HelicoBlot 2.1 (GENELABS DIAGNOSTICS, Singapore). All tests were performed according to their manufacturer′s instructions. The percentage of agreement was evaluated for each of the assays. Equivocal results were excluded.
Statistical analysis
SPSS package (v. 11.5) was used for statistical analysis. A receiver operating curve (ROC) analysis was applied for pairs of sensitivity and specificity to find the best diagnostic value. In order to determine the agreement between different assays, Cohen′s kappa values were calculated. These values were interpreted as follows: 0 to 0.2 (poor), 0.21 to 0.4 (fair), 0.41 to 0.6 (moderate), 0.61 to 0.8 (good), 0.81 to 0.99 (very good) and 1 (perfect agreement).
Results
The mean age of the studied population ( n = 199) was 38.6 ± 15 years ranging between 18 and 85, including 87 male and 112 female subjects.
Hp positive and negative sera, as confirmed by gold standard tests, were used for standardisation of the assay. This standardization resulted in optimal concentrations and dilution rates for the coating antigen, primary and secondary antibodies as 5 μg/mL, 1:100 and 1:80,000, respectively.
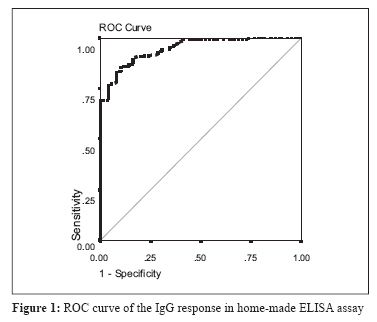
The appropriate cut off value was calculated via ROC curve using confirmed Hp-positive and negative sera [Figure - 1] which yielded a cut-off value of 0.4 with the equivocal range of 0.35 to 0.45. According to these values, serological criteria were calculated for the home-made kit after exclusion of border line values [Table - 1]. Therefore, the accuracy, sensitivity, specificity, PPV and NPV of the home made kit were 91.8, 92.2, 90.4, 97 and 77.5%, respectively.
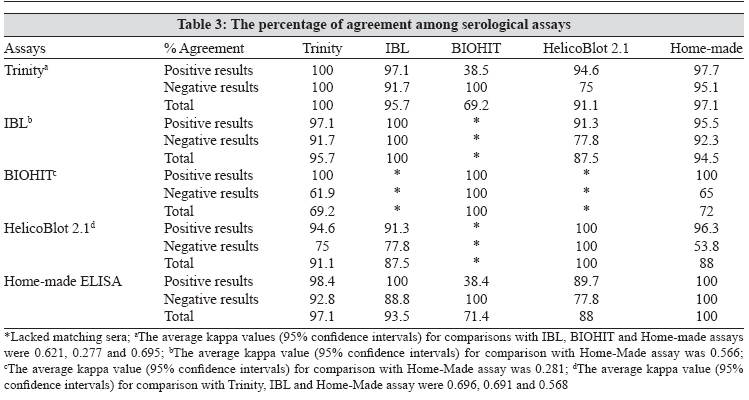
Three available commercial ELISA kits and one western blot kit were used for comparison. Serological criteria for these assays are indicated in [Table - 2]. Among these serological kits, the highest and lowest criteria belonged to Trinity and BIOHIT ELISA kits respectively. The degree of agreement between each pair of kits was also calculated [Table - 3]. There was an overall "good" agreement between the home made ELISA kit, Trinity and IBL kits (the average kappa values ranged from 0.566 to 0.695) but BIOHIT kit showed a "poor" agreement with Trinity and the home-made kits (the average kappa values were 0.277 and 0.281).
Discussion
The majority (up to 85%) of the Iranian adult population are Hp seropositive [7] which may be due to acquiring Hp infection in the early years of life such that inclusion of true negatives in sero-epidemiological studies is quite problematic. Screening this population to determine Hp seropositive cases for an effective treatment and monitoring the success of therapy can be an appropriate approach in devising Hp eradication strategies and follow-ups for such a highly infected population.
Although there are several commercially available ELISA kits for detection of Hp infection with high serological criteria, adjusted values for the target populations drop below these values. For instance, sensitivity and specificity of HM-CAP in US has been reported as 98.4 and 96.4% [13] and in China as 72.7 and 68.4% by Leung et al . [14] Thus, it can be postulated that these assays are not uniformly effective in different geographic regions and their criteria are lower in East Asia than in the Western countries. Accordingly, in this study we found desirable high sensitivity values for all tested kits except BIOHIT ELISA assay. As for specificity, the obtained values were similar and in the range of 88.5-100%. The accuracies were also compared and showed that the overall accuracy of BIOHIT ELISA kit is much lower than the other assays. Calculated kappa values [Table - 3] indicate there is an overall moderate to good agreement between the home-made kit and imported ones. Discrepancies among the sensitivity of these assays might be associated with the presence of peptic ulcers, [15] increased age of patients [16] or rarely can be due to the presence of an acute Hp infection (a recent infection) before induction of a systemic antibody response. The low specificity may be due to improper sampling or reasons which may drop the load of infection to levels below threshold of detection of our gold standard tests including the presence or progress of atrophy and intestinal metaplasia [17] and previous antibiotic treatments. The exact reasons for these discrepancies should be investigated in details among the studied group of patients.
The extensive heterogeneity among isolated Hp strains from different areas even within one country is repeatedly reported. [12],[18] The authors have shown significant molecular heterogeneity between Iranian and western Hp strains in some Hp conserved and non conserved genes, [19],[20] which can induce different immune responses and emphasises the need for using native (local) antigens in developing an ELISA assay for detection of seroreactivity toward this microorganism. Therefore, Hp detection using imported ELISA kits may yield false results and their criteria coming from the country of origin (sensitivity, specificity and accuracy) cannot be trusted for the country of application. In other words, a significant heterogeneity between isolated Hp strains from different geographic regions, cross reactivity with other enteric pathogens are some possible reasons for uncertain results in determining Hp infection via imported ELISA kits. Therefore, high serological criteria of an ELISA kit may not be reproduced in another population. In this study immunologic criteria for imported kits were lower than those reported from their original country. The observed discrepancies reveal that for obtaining the actual criteria of imported kits, they should be recalculated using true positive and negative sera through drawing new ROC curves in the country they are imported in.
This study is strengthened by incorporation of a cocktail of local strains in the home-made kit which increases the chance of host serum antibody detection and simultaneous blood, breath and gastric sampling reduces potential inconsistencies. It is however limited by the fact that the elderly population may possess lower antibody titers which may produce false negative results. Furthermore, it has been reported that the cut-off value for symptomatic patients may be above that of the asymptomatic population thus overlooking truly positive Hp infected asymptomatic individuals with lower antibody titers.
The above discrepancies and the comparable serological criteria of the home made ELISA kit to that of the most efficient imported kit (Trinity), plus its significant cost benefit (cost per sample of less than half), while incorporating local strains matching those infecting the population recommends this kit as a suitable substitution for the commercially imported kits in screening Hp infection in Iran.
Acknowledgment This study was funded by a generous grant from Medical Biotechnology Network supported by the Ministry of Health and Medical Education of Iran.
References
| 1. | Warren JR. Unidentified curved bacilli on gastric epithelium in active chronic gastritis. Lancet 1983;1:1273-5. Back to cited text no. 1 |
| 2. | International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans, vol. 61. Schistosomes, Liver Flukes and Helicobacter pylori . IARC: Lyon, France; 1994. p. 177-241. Back to cited text no. 2 |
| 3. | Prinz C, Schwendy S, Voland P. Helicobacter pylori and gastric cancer: Shifting the global burden. World J Gastroenterol 2006;14:5458-64. Back to cited text no. 3 |
| 4. | Skowasch D, Jabs A, Andrie R, Dinkelbach S, Schiele TM, Wernert N, et al . Pathogen burden, inflammation, proliferation and apoptosis in human in-stent restenosis. Tissue characteristics compared to primary atherosclerosis. J Vasc Res 2004;41:525-34. Back to cited text no. 4 |
| 5. | Nilson H, Pietroiusti A, Gabrielli M, Assunta Zocco M, Gasbarrini G, Gasbarrini A. Helicobacter pylori and extragastric disease-other Helicobacters. Helicobacter 2005;10:54-65. Back to cited text no. 5 |
| 6. | Telford JL, Ghiara P, Dell'Orco M, Comanducci M, Burroni D, Bugnoli M, et al . Gene structure of the Helicobacter pylori cytotoxin and evidence of its key role in gastric disease. J Exp Med 1994;179:1653-8. Back to cited text no. 6 [PUBMED] [FULLTEXT] |
| 7. | Massarrat S, Saberi-Firoozi M, Soleimani A, Himmelmann GW, Hitzges M, Keshavarz H. Peptic ulcer disease, irritable bowel syndrome and constipation in two populations in Iran. Eur J Gastroenterol Hepatol 1995;7:427-33. Back to cited text no. 7 [PUBMED] |
| 8. | Jafarzadeh A, Rezayati MT, Nemati M. Specific serum immunoglobulin G to H. pylori and CagA in healthy children and adults (South-east of Iran). World J Gastroenterol 2007;13:3117-27. Back to cited text no. 8 |
| 9. | Vorobjova T, Grunberg H, Oona M, Maaroos HI, Nilsson I, Wadstrom T, et al . Seropositivity to Helicobacter pylori and CagA protein in schoolchildren of different ages living in urban and rural areas in southern Estonia. Eur J Gastroenterol Hepatol 2000;12:97-101. Back to cited text no. 9 |
| 10. | Anderson LP. The antibody response to Helicobacter pylori infection and the value of serologic tests to detect H. pylori and for post- treatment monitoring. In : Stewart Goodwin C, Worsley BW, editors. Helicobacter pylori biology and clinical practice. CRC Press: Boca Raton; 1993. p. 285-305. Back to cited text no. 10 |
| 11. | Leung WK, Chow TP, Ng EK, Chan FK, Chung SC, Sung JJ. Validation of a new immunoblot assay for the diagnosis of Helicobacter pylori in the Asian population. Aliment Pharmacol Ther 2001;15:423-8. Back to cited text no. 11 |
| 12. | Figueiredo C, Quint W, Nouhan N, van der Munckhof, Herbrink P, Scherpenisse J, et al . Assessment of Helicobacter pylori vacA and cagA genotypes and host serological response. J Clin Microbiol 2001;39:1339-44. Back to cited text no. 12 |
| 13. | Marchildon PA, Ciota LM, Zamaniyan FZ, Peacock JS, Graham DY. Evaluation of three commercial enzyme immunoassays compared with the 13C urea breath test for detection of Helicobacter pylori infection. J Clin Microbiol 1996;34:1147-52. Back to cited text no. 13 [PUBMED] [FULLTEXT] |
| 14. | Leung WK, Ng EK, Chan FK, Chung SC, Sung JJ. Evaluation of three commercial enzyme-linked immunosorbent assay kits for diagnosis of Helicobacter pylori in Chinese patients. Diagn Microbiol Infect Dis 1999;34:13-7. Back to cited text no. 14 [PUBMED] [FULLTEXT] |
| 15. | Xia HH, Kalantar JS, Wyatt JM, Adams S, Cheung K, Eslick GD, et al . High sensitivity and specificity of a laboratory-based serological test, pylori DTect ELISA, for detection of Helicobacter pylori infection. Diagn Microbiol Infect Dis 2000;36:69-74. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Liston R, Pitt MA, Banerjee AK. IgG ELISA antibodies and detection of Helicobacter pylori in elderly patients. Lancet 1996;347:269-70. Back to cited text no. 16 |
| 17. | Asaka M, Sugiyama T, Nobuta A, Kato M, Takeda H, Graham DY. Atrophic gastritis and intestinal metaplasia in Japan: Results of a large multicenter study. Helicobacter 2001;6:294-9. Back to cited text no. 17 [PUBMED] [FULLTEXT] |
| 18. | Alm RA, Ling LS, Moir DT, King BL, Brown ED, Doig PC, et al . Genomic- sequence comparison of two unrelated isolates of the human pathogen Helicobacter pylori . Nature 1999;397:176-80. Back to cited text no. 18 [PUBMED] [FULLTEXT] |
| 19. | Mohammadi M. Genotype and strains of Iranian Helicobacter pylori strains based on PCR-RFLP of conserved and non-conserved genes. Bull Soc Pathol Exot 2000;93:224-6. Back to cited text no. 19 [PUBMED] |
| 20. | Mohammadi M, Oghalaie A, Mohajerani N, Massarrat S, Nasiri M, Bennedsen M, et al . Prevalence of Helicobacter pylori vacuolating cytotoxin and its allelic mosaicism as a predictive marker for Iranian dyspeptic patients. Bull Soc Pathol Exot 2003;96:3-5. Back to cited text no. 20 [PUBMED] |
Copyright 2008 - Indian Journal of Medical Microbiology
The following images related to this document are available:
Photo images
[mb08038t2.jpg]
[mb08038t3.jpg]
[mb08038t1.jpg]
[mb08038f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}