 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
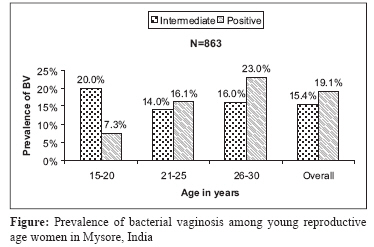
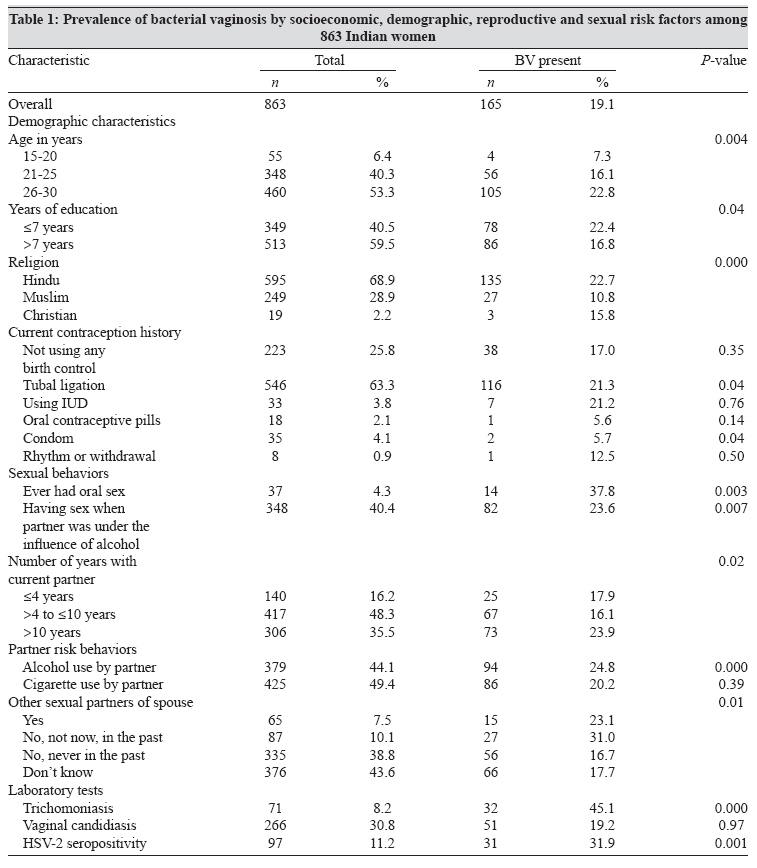
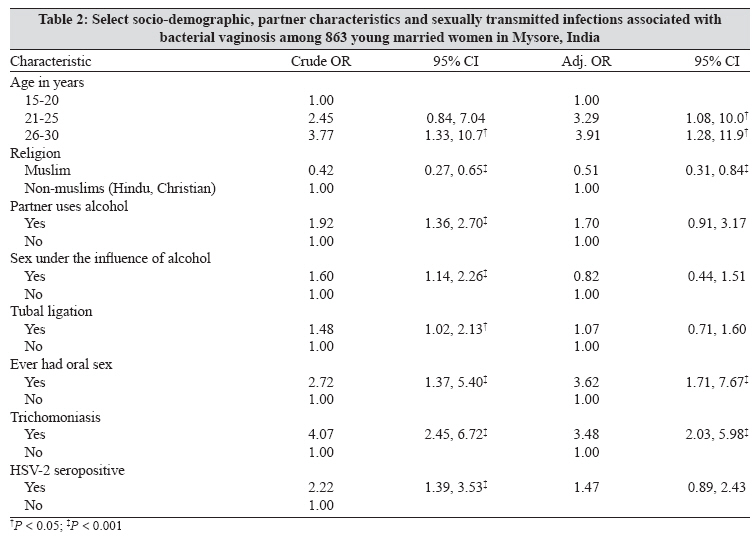
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 132-137 Original Article Prevalence and correlates of bacterial vaginosis among young women of reproductive age in Mysore, India Madhivanan P, Krupp K, Chandrasekaran V, Karat C, Arun A, Cohen CR, Reingold AL, Klausner JD Division of Epidemiology, School of Public Health, University of California, Berkeley, USA; Public Health Research Institute, Mysore - 570020, India Date of Submission: 15-Aug-2007 Code Number: mb08039 Abstract Purpose: Bacterial vaginosis (BV) is the most common cause of abnormal vaginal discharge among women of childbearing age and is associated with STI/HIV and adverse birth outcomes. The objective of this study was to determine the prevalence and correlates of BV among young women of reproductive age in Mysore, India. Keywords: Bacterial vaginosis, correlates, epidemiology, India, prevalence, sexually transmitted infections Bacterial vaginosis (BV) is the most common cause of abnormal vaginal discharge among women of childbearing age and is associated with low birth weight infants (LBW) and preventable preterm births. Various studies across the world have shown that women with BV are more likely to be co-infected with herpes simplex virus type-2 (HSV-2), Trichomonas vaginalis , Neisseria gonorrhoeae and HIV. [1],[2],[3],[4] Some studies have found a relationship between BV and high-risk behaviours associated with sexually transmitted infections (STIs) such as early sexual debut and multiple sex partners. [5] High co-infection rates with other STIs raise the possibility that BV may either increase susceptibility to STI or share a common pathway with other STIs. [1],[4] BV is of special public health concern in India because of the high burden of reproductive and pregnancy-related morbidity. Research on BV in India is sparse and mainly limited to a few states. [6],[7],[8],[9],[10] To date, there are only two studies on the prevalence of BV in the state of Karnataka. [9],[10] Because these studies had small sample sizes and one study diagnosed BV using Papanicolaou smears, [9] it is difficult to interpret the findings. This study examined the prevalence and potentially modifiable risk factors for BV in young women of reproductive age and their male sex partners in Mysore, India. Materials and Methods Study population Laboratory methods Data analysis Results Of the 898 women enrolled, a diagnosis for BV was available among 863 (96%) because 35 slides were unreadable (inadequate material, over-stained or missing). The 35 women for whom a diagnosis of BV was unavailable did not differ from the study participants in age, education level, occupation or marital status. All women in the study reported being ever married, with 10 women living with another partner, four widowed and four separated. Almost half (49%) of the participants had more than five years of education, but 26% did not receive any schooling. Seventy-four percent reported that their sole occupation was performing household chores and taking care of children. In addition to running a household, 20% worked as unskilled labourers in agriculture, rolling incense sticks or beedis , and 6% had other occupations. No women reported being involved in commercial sex work. Among the male partners, 45% were unskilled labourers (e.g., agriculture, construction, truck loading, cleaning, etc.), 43% performed skilled jobs (e.g., electricians, carpenters, technicians, etc.), and another 11% were drivers (lorry, taxi or auto rickshaws). Women reported a mean of five members living in each household, and 82% reported less than or equal to 4000 INR as their total monthly household income. Sixty percent of the participants had their sexual debut before 18 years of age. Only 18 women (2%) reported more than one sex partner in their lifetime, and only four of those reported a new sex partner in the preceding three months. The median number of times a woman reported having had vaginal intercourse in the prior three months was 24 (IQR = 36-12). Condom use was low, with 94% reporting never having used a condom and only 4% reporting consistent condom use. Thirty-seven (4.3%) women reported ever having had oral sex, of whom 34 had it in the prior three months. Reversible methods of contraception were rarely used. A majority of the participants (63%) had undergone tubal ligation. None of the women were concurrently using multiple contraception methods. Of the 863 women, 165 were diagnosed with BV (19.1%, 95% CI: 16.5-21.8%), 133 women (15.4%, CI: 13.0-17.9%) had intermediate flora and 565 (65.4%, CI: 62.1-68.6%) had normal flora [Figure - 1]. Women with BV were on an average older, non-Muslim, lived with their current partner for more than 10 years, had undergone tubal ligation and reported having had oral sex. These women also reported having partners who had other sex partners and drank alcohol [Table - 1]. Cigarette use and douching were not reported by any study participant. Unadjusted logistic regression analyses showed several characteristics of participants that were associated with BV [Table - 2]. Women who were older in age, non-Muslim (Hindu or Christian), having undergone tubal ligation, having partners who used alcohol or had other sex partners had increased odds of being diagnosed with BV. BV was also significantly associated with prevalent trichomoniasis and HSV-2 seropositivity. In multivariable analyses, after adjusting for factors that were significant in the unadjusted analyses, only three factors remained significantly associated with the presence of BV. The relative odds of being diagnosed with BV for Muslim women was 0.5 (95% CI: 0.3-0.9) as compared to non-Muslim women. In addition, having prevalent trichomoniasis (AOR: 3.5, 95% CI: 2.0-6.2) or a partner who drank alcohol (AOR: 1.6, 95% CI: 1.1-2.3) was significantly associated with BV. Discussion Since India has a high burden of reproductive morbidity, and BV has been documented as a risk factor for both adverse birth outcomes and HIV, this study investigated potentially modifiable behavioural and biological risk factors for BV. The prevalence of BV in this sample, at 19%, was in the range of previous findings for other populations in India. [6],[14] In unadjusted analyses, BV was associated with older age in this study. Some researchers have previously reported that the condition is more common among younger women, [15] while others have found that risk for BV increases with age. [16],[17] We hypothesize that, in this population, age is a proxy for cumulative sexual activity, which has been found to be associated with BV. Interestingly, although the proportion of women with BV increased with age, a higher percentage of younger women (15-20 years of age) were found to have intermediate flora by Nugent score [Figure - 1]. This seems counterintuitive because one would assume that a higher number of women with intermediate scores should also be reflected in elevated levels of BV among the same age group. It appears that Nugent score may misclassify disturbed vaginal flora as a stage in BV pathogenesis in younger women. In India, this may have important implications because women in the 15-20 year age range are at higher risk for STI and bad birth outcomes. Because we had a relatively small number of women in this age category, more research is needed to understand the performance of Nugent′s score among younger women for the diagnosis of BV. Religion was the only socio-demographic variable that remained significantly associated with BV after adjusting for other correlates in the multivariable analyses. In our study, non-Muslim women (Hindus and Christians) had 1.9 times the odds of having BV as compared to Muslim women. Another study in Africa showed similar findings. [18] Since we did not collect information on certain risk factors, such as genital hygiene practices that are known to be associated with BV and may vary by religion, [15] additional research is needed to better understand the socio-cultural risk factors surrounding this condition. Other socio-demographic known risk factors such as marital status, douching and smoking were not associated with BV in our population. [19],[20],[21],[22] Consistent with other research, trichomoniasis was associated with BV [8],[18] in our study. The cross-sectional nature of this analysis did not allow us to establish temporality of these infections. It is plausible that T. vaginalis infection alters the vaginal ecology and facilitates the development of BV, or that women with BV have lost natural protection against genital tract infections leading to the acquisition of STIs like T. vaginalis infection. The mechanisms underlying these relationships are not well understood, and warrant further investigation. We had hypothesized that high-risk sexual behaviors in men increased the odds of BV in their female sex partners. Although we found that partner age, education, occupation (data not shown) and smoking status were not associated with BV, having a male partner who used alcohol or had other sex partners were found to be significantly associated with BV. [17] Although our study does not have adequate information on partner sexual behaviours, our findings do suggest that male partner characteristics may play a role in the development of BV. There are several limitations in our study. Because the analyses were cross-sectional in nature, we cannot infer any causal association between STI and BV. In addition, risk factors were self-reported, and it is possible that there was under-reporting and misclassification of risk behaviors. The survey involved the collection of temporally distant and sensitive sexual behaviors, as well as information on women′s sex partners, so there is a possibility of measurement error that may lead to residual confounding obscuring the relationships. Although oral sex was found to be associated with BV in the bivariate analyses, we did not include it in the regression model because we had not collected information that would help us differentiate receptive oral sex from giving oral sex. Because receptive oral sex has been shown to be a risk factor for BV, further research is needed to better understand this association in Indian women. Another limitation of this study was the potential for selection bias as a non-random sample was used in the study; and the findings may not be generalizable to other populations. Despite these limitations, the possible links of BV with trichomoniasis, being a non-Muslim and partner′s alcohol use warrant further investigation given the high burden of reproductive morbidity and poor birth outcomes in India. Furthermore, because there is strong evidence in literature that BV is associated with STIs including HIV, further studies are needed to understand the potential role of screening and treatment of BV in STI/HIV prevention programs. Acknowledgements PM was supported by the Fogarty AIDS International Training and Research Program (Grant 1-D43-TW00003-16). The authors would like to thank Drs. Mothi Sarvode, Mahesh Kumar, SC Karat, Srikanth and Jeanne Moncada for technical support and all NGOs and study participants involved in the study. BioMed Diagnostics, Focus Technologies and Cipla are thanked for their generous donations for the study.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08039t1.jpg] [mb08039t2.jpg] [mb08039f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}