 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
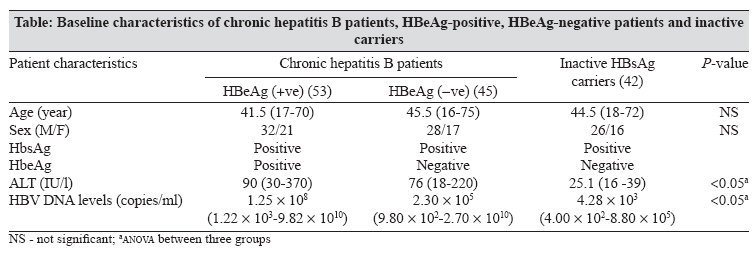
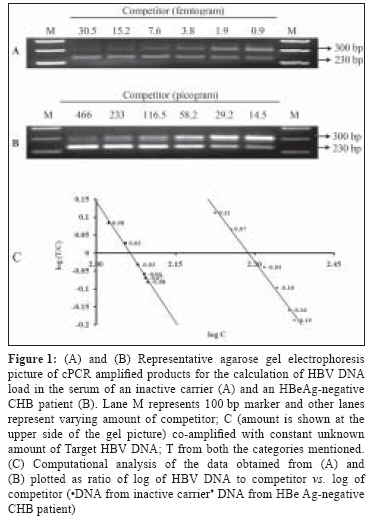
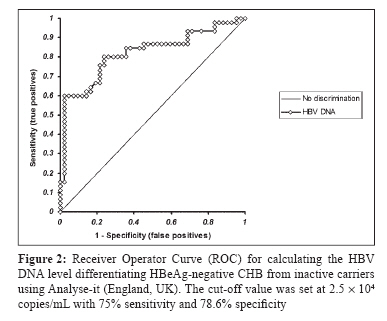
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 138-142 Original Article Diagnosing different stages of hepatitis B infection using a competitive polymerase chain reaction assay Changotra H, Dwivedi A, Nayyar AK, Sehajpal PK Molecular Diagnostic Laboratory, Department of Molecular Biology and Biochemistry, Guru Nanak Dev University, Amritsar - 143 005 Date of Submission: 14-May-2007 Code Number: mb08040 Abstract Purpose: Different stages of hepatitis B virus (HBV) infection can be defined by serum HBV DNA levels. This study attempts to (1) investigate serum HBV DNA levels in inactive carriers and patients with chronic HBV (CHB) infection and (2) define cut-off value between inactive carriers and HBeAg (precore antigen of HBV) negative CHB patients in Indian population. Keywords: Chronic hepatitis B, HBeAg, HBsAg, HBV DNA, inactive carriers, quantitation Approximately, one-third of the world population has serological evidence of the past or present Hepatitis B virus (HBV) infection resulting in 400 million chronically infected people. [1] This could lead to a variety of clinical outcomes ranging from an apparently healthy asymptomatic carrier state to acute or chronic liver disease, including cirrhosis and hepatocellular carcinoma. [1],[2] Persistent presence of hepatitis B surface antigen (HBsAg) for at least six months defines the chronic hepatitis B (CHB) carrier state. Conventionally, presence of secretory version of a HBV core protein, the e antigen (HBeAg), is associated with high viral load and serves as a marker for viral replication. [3] HBeAg seroconversion (HBeAg negative and anti-HBe) is associated with liver disease remission and marks the transition from chronic hepatitis B to the asymptomatic HBsAg carrier state, which does not show the clinical symptoms of the disease. At the time of HBeAg seroconversion, a small percentage of patients continue to show raised alanine aminotransferase (ALT) and serum HBV DNA levels. [3] This group of patients is called as HBeAg negative CHB which continues to have liver damage but due to frequent changes of ALT levels, becomes difficult to differentiate from inactive carriers. [1],[4] In the past decade, detection and quantification of HBV infection in patients has drastically evolved due to the advent of molecular tools. This has immensely helped in understanding the pathogenesis and the natural course of HBV infection [3] and simultaneously, raised new predicaments and clinically relevant questions. To address some of the issues, a research workshop held at National Institute of Health (NIH), USA, on hepatitis B recommended the use of a new term "inactive HBsAg carrier state" instead of healthy asymptomatic carriers. Additionally, it was proposed that this class of HBV carriers is better defined by an arbitrary HBV DNA level below 10 5 copies/mL of the serum [5] and the patients having levels more than this value should undergo antiviral treatment (AVT), irrespective of the HBeAg status contrary to earlier belief. Following this, various investigators have attempted to validate the proposed cut-off limits for differentiating these two groups of carriers and found that a lower threshold value might be more relevant in their populations. [6],[7],[8],[9] Such a study turns out to be imperative in a country like India where no such data exists and the burden of this virus is second highest in the world. [10] The present study attempts to fill this void. Materials and Methods Patients, liver function tests and viral markers Collected serum samples were screened for the presence of HBsAg and HBeAg serological markers using commercially available kits (Abbott Laboratories, North Chicago, IL). Serum ALT levels were measured using a commercial kit (Bayer Diagnostics, USA) for which the upper normal limit is 40 IU/l. HBV DNA isolation Quantitative detection of HBV DNA Statistical analysis Results The demographic and clinical data of the three studied groups were compared with respect to sex, age, ALT and HBV DNA levels [Table - 1]. HBV DNA levels were estimated employing cPCR assay as described in the section, materials and methods. [Figure - 1] depicts a representative agarose gel electrophoresis picture of the co-amplified products in case of an inactive carrier (A) and an HBeAg-negative CHB patient (B) and its computational analysis (C) for the calculation of viral load, which was observed to be 7.55 x 10 3 copies/mL in case of (A) and 2.27 x 10 8 copies/mL in (B). The three studied groups had predominantly male population with similar median age. ALT levels differed statistically in these groups (ANOVA; P < 0.05). Baseline serum HBV DNA levels among the HBeAg-negative patients were significantly lower than the HBeAg-positive patients (median; 2.30 x 10 5 vs. 1.25 x 10 8 copies/mL; P < 0.05) and significantly higher than the inactive carriers (median; 2.30 x 10 5 vs. 4.28 x 10 3 copies/mL ; P < 0.05). HBV DNA levels overlapped extensively between HBeAg-negative CHB patients and inactive carriers; despite this the levels between the two groups differed statistically. The optimal HBV DNA cut-off level on Receiver Operator Curve discriminating HBeAg-negative CHB and inactive carriers was 2.50 x 10 4 copies/mL, with 75.60% sensitivity and 78.60% specificity [Figure - 2]. Nine out of forty-two (21.42%) of inactive carriers were above and 24.44% (11/45) of HBeAg-negative CHB patients were below this value. However, 1/42 (2.38%) of the inactive carriers and 27/45 (60.00%) HBeAg negative CHB were respectively, above and below the NIH cut-off value of 10 5 copies/mL . Discussion HBV-infected patients show variety of clinical symptoms ranging from an apparently healthy inactive carrier state to fulminant hepatitis or chronic liver disease, including cirrhosis and hepatocellular carcinoma. [1],[2] Inactive carriers have lower risk of progression to liver cirrhosis as well as to liver cancer compared to chronic hepatitis B patients with the latter benefiting from the anti-viral treatment. [4] One of the most common ironies in case of chronic hepatitis B patients is the differentiation between HBeAg-negative CHB cases from the inactive carriers as they share their serological profile. [14] Viral load quantification plays a vital role in the better management of this dreadful pathogen [15] as it is helpful in defining the state of infection, [16] designing drug regimen [17] as well as in monitoring antiviral treatment. [18] Consequently, the present study was attempted to define the serum HBV DNA cut off levels differentiating the three studied states of HBV infection relating to Indian population. In our study, the observed median HBV DNA levels in different stages of HBV infection were different from the ones reported earlier on other populations of the world. [6],[7],[8],[9] However, the median HBV DNA level for the HBeAg-positive patients was statistically higher than the HBeAg-negative ones and similar trend was observed between the HBeAg-negative CHB patients and the inactive carriers [Table - 1]. Various studies on different populations of the world suggest that a lower cut-off value appears to be a better marker for differentiating HBeAg-negative CHB patients from the inactive carriers [6],[7],[8],[9] as compared to NIH recommended value of 10 5 copies/mL . In the present study also, we found 2.5 x 10 4 copies/mL [Figure - 2] as a better limit to differentiate the said categories of individuals. On categorising the patients according to NIH guidelines, 60.0% of HBeAg-negative-CHB patients were below and 2.4% of inactive carriers were above the cut off value. Similarly, according to 2.5 x 10 4 copies/mL value, 24.4% of HBeAg-negative CHB and 21.4% of inactive carriers were below and above this value, respectively. The data of inactive carriers in this study is in accord with earlier report by Martinot-Peignoux et al. , [19] according to which 98% of the inactive carriers have HBV DNA levels below the NIH cut-off level and 97% of them were found to be stable during follow-up. HBV DNA levels of HBeAg-negative CHB patients could not be compared, as they were not included in their study. However, according to a study by Chu et al. , [6] NIH recommended value excluded 45.0% of HBeAg-negative CHB patients in their population. Similarly, Hoe et al. , [7] observed while studying Korean population, that NIH value exclude 40.4% HBeAg-negative CHB patients and additionally, 20.0% of the inactive carriers were above this value. Evidently, HBV DNA levels in Indian HBsAg-positive population are lower in both the cases. These variations may be attributed to ethnic differences [20] between the population studied and/or an outcome related to the prevalent genotypes in the respective parts of the world. [21] So far, eight HBV genotypes (A through H) have been identified which vary in their pathogenicity and geographical distribution. [21] In conclusion, HBV DNA levels vary significantly in different states of the infection, which is helpful in diagnosing the state of infection and in turn help in designing the drug regimen. Cut-off value to classify HBeAg-negative CHB patients and inactive carriers was set at 2.5 x 10 4 copies/mL for Indian population though there was enormous overlapping of HBV DNA levels. Furthermore, such studies on large samples are needed to validate this value. This value shall be imperative in the better management of this dreadful disease in our part of the world. Acknowledgements HC is thankful to Council of Scientific and Industrial Research, New Delhi, India, for the award of a Senior Research Fellowship.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08040f2.jpg] [mb08040f1.jpg] [mb08040t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}