 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
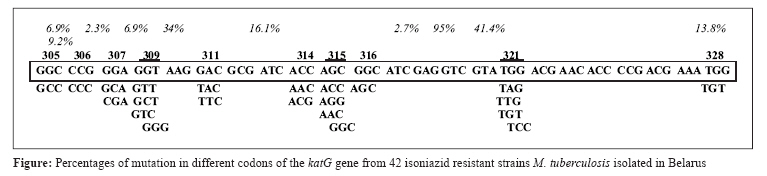
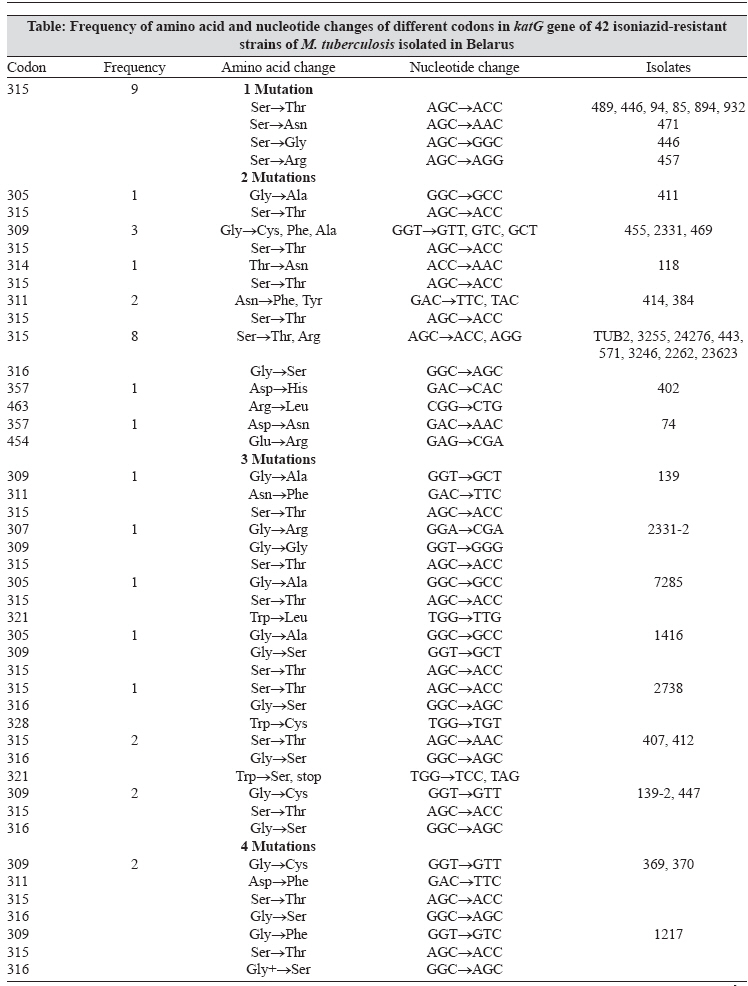
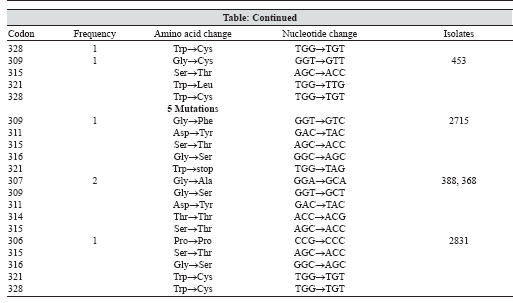
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 143-147 Brief Communication Detection of mutation in isoniazid-resistant Mycobacterium tuberculosis isolates from tuberculosis patients in Belarus Bostanabad SZ, Titov LP, Bahrmand A, Nojoumi SA Belarusian Research Institute for Epidemiology and Microbiology (BRIEM), Filimonova 23, Minsk, Belarus, and Molecular Genetic Laboratory of Mycobacteria, Pasteur Institute of Iran (PII), St. Paster 13164, Tehran Date of Submission: 14-Apr-2007 Code Number: mb08041 Abstract The aim of this study was to investigate the frequency, location and type of katG mutations in Mycobacterium tuberculosis strains isolated from patients in Belarus. Forty two isoniazid-resistant isolates were identified from sputum of 163 patients with active pulmonary tuberculosis. Drug susceptibility testing was determined by using CDC standard conventional proportional method and BACTEC system. Standard PCR method for detection of isoniazid resistance associated mutations was performed by katG gene amplification and DNA sequencing. Most mutations were found in katG gene codons 315, 316 and 309. Four types of mutations were identified in codon 315: AGC→ACC ( n = 36) 85%, AGC→AGG ( n = 1) 2.3%, AGC→AAC ( n = 2) 4.7%, AGC→GGC ( n = 1) 2.3%. One type of mutation was found in codon 316: GGC→AGC ( n = 18)41.4%, four types of mutations were detected in codon 309: GGT→GGT ( n = 7)16.1%, GGT→GCT ( n = 4)9.2%, GGT→GTC ( n = 3)6.9%, GGT→GGG ( n = 1)2.7%. The highest frequency of mutations sharing between primary and secondary infections was found in codon 315.Keywords: katG gene, mutation, M. tuberculosis, Belarus The emergence of drug-resistant strains of M. tuberculosis (MTB) is an increasing problem in developed and developing countries. [1],[2],[3],[4],[5] Belarus is in southern endemic region of Europe with 20 to 30% multiple-drug resistant (MDR) isolates among 50.6 tuberculosis cases per 100,000 population. [6] Resistance to isoniazid is increasing in Belarus because 88% of hospitalized patients with drug resistant tuberculosis in Institute of Pulmonology and Tuberculosis (Belarus-Minsk, Magilev, Brest, Gomel, Horodna and Vitebsk] demonstrated resistance to at least isoniazid and rifampicine. [6],[7] In United States, approximately 13% of isolates from new tuberculosis cases are resistant to one or more of the first-line anti tuberculosis chemotherapy and 1.6% of cases are resistant to both isoniazid and rifampicin, defined as MDR tuberculosis. [3],[8],[9] Recent worldwide surveillance has demonstrated that drug-resistant strains are now widespread and are reaching alarmingly high levels in certain countries. MDR-TB is potentially untreatable transmissible disease associated with high mortality. [2],[3],[8],[10] Resistance to isoniazid is associated with a variety of mutations affecting one or more genes such as those encoding catalase-peroxidase (katG) . [11] KatG gene is the most commonly targeted region with majority of mutations occurring in codon 315 in 30-90% of isoniazid-resistant strains depending on geographical distribution. Extensive studies have demonstrated that isoniazid resistance is most frequently associated with a specific mutation in katG (codon 315), a gene that encodes the catalase-proxidase enzyme in M. tuberculosis. [4] The observation, that most isoniazid-resistant M. tuberculosis strains did not indicate gross katG deletions suggested the need to more precisely analyse the structure of katG present in resistant M. tuberculosis isolates. Several groups recently reported that many isoniazid-resistant strains contain missense, other types of mutations and seldom demonstrated to have deletion in katG gene. [5],[9],[13] PCR amplification and DNA sequencing analysis detects mutations within katG gene and is predictive of drug resistance with the potential to provide rapid detection for isoniazid-resistant isolates of M. tuberculosis . Scope of this work was to determine mutations in codons of katG gene causing resistance to isoniazid among M. tuberculosis isolates in Belarus. Materials and Methods One hundred and sixty three strains of M. tuberculosis isolated from sputum of patients with active pulmonary tuberculosis in different geographic regions of Belarus (Minsk 11, Mogilev 9, Gomel 3, Grodho 3, Brest 8, Vitebsk 8) from December 2004 to May 2005 were included in the study. All 163 tuberculosis patient cases had proven registration of clinical diagnostic exanimations, such as chest X-ray, PPD, cough, weight loss, gender etc. Patient sputum samples was cultured on Lowenstein-Jensen medium and grown colonies that were identified to the species level using TCH (2-thiophene carboxylic acid) and PN99B (paranitrobenzoic acid) selective media or by standard biochemical procedures. Four isoniazid sensitive isolates were used as negative control. [10] Antimicrobial drug susceptibility testing (AMST) was performed using CDC standard conventional proportional method [rifampicine (Rif) - 40 mg/L, isoniazid (INH) - 0,2 mg/L, ethambutol (EMB) - 2 mg/L, ethionamide (ETH) - 20 mg/L, streptomycin (SM) - 4 mg/L and kanamycin (K) - 20 mg/L], [8] in addition to BACTEC system with drug concentration of isoniazid 0.1 μg/mL and rifampicine 2.0 μg/mL. DNA extraction was performed using manufacture procedure Fermentas kit′s (K512). DNA extracted from standard strain of Mycobacterium H37RV was used as control. A 210-bp and 750-bp segment of the katG gene was amplified by PCR using the following synthetic oligonucleotide primers; katG F 5-GAAACAGCGGCGCTGGATCGT-3, katG R 5 - GTTGTCCCATTTCGTCGGGG-3 for 210-bp and katG F 5-CGGGATCCGCTGGAGCAGATGGGC-3 and katG R 5-CGGAATTCCAGGGTGCGAATGACCT-3 for 750-bp. [5] The following thermocycler parameters were applied with initial denaturation at 95°C for 5 minutes; 36 cycles of denaturation at 94°C for 1 minute; primer annealing at 56°C for 1 minute; extension at 72°C for 1 minute; and a final extension at 72°C for 10 minute. The PCR product was amplified and purified again and checked on the gel electrophoresis. The final purified DNA obtained was used for sequencing. For DNA sequencing the 209-bp and 750-bp fragment of katG gene was amplified by PCR using forward and reverse primers; 33 cycles of denaturation at 94°C for 30 seconds; primer annealing at 48°C for 45 seconds; extension at 60°C for 4 minutes. katG gene fragments were sequenced using the Amersham auto sequencer and Amersham Pharmacia DYEnamic ET Terminator Cycle Sequencing Premix Kits. The purified katG gene fragments (4 isoniazid sensitive and standard strains of M. tuberculosis H37RV were used as controls) were sequenced. Alignment of the DNA fragments (katG) was carried out with the help of MEGA and DNAMAN software (Gen bank_ PUBMED/BLAST) and compared by standard strains of CDC1551, H37RV. The Blast 2 sequences computer program was used for DNA sequence comparisons (http://www.ncbi.nlm.nih.gov/BLAST/). Results Out of 163 strains, 42 (68.5%) were identified as resistant to isoniazid, rifampicin, and streptomycin and eight isolates (28%) were resistant to ethambutol. Mono-resistance to isoniazid was observed in four isolates (14%). From 163 isolates, 121 were sensitive to isoniazid in which four sensitive isolates were used as control in sequencing. No mutations were detected in four isolates sensitive to isoniazid in 210-bp and 750-bp region of katG gene. Mutations were observed in codons 305, 306, 307, 314, 316, 321, 328, 315, 316,357, 454,463 and 309 of affected fragments in 210-bp and 750-bp of katG gene. Ninety five percent of all isolates showed mutation in codon 315, whereas 40% of all mutations of different types were observed in codon 315: AGC→ACC (Ser→Thr) 36%, AGC→AGG (Ser→Arg) 0.9%, AGC→AAC (Ser→Asn) 1.8%, AGC→GGC (Ser→Gly) 0.9%. Four types of mutations were detected in codon 309: GGT→GTT (Cys→Phe) 6.3%, GGT→GCT (Cys→Ser) 3.6%, GGT→GTC (Cys→Phe) 2.7%, GGT→GGG (Cys→Thr) 0.9% and one in 316 GGC→AGC (Gly→Ser) 14.4%. In this study, 75% of all isolates demonstrated to have mutations in codons 309 ( n = 15, 34%) and 316 ( n = 18, 41.4%) which might represent second most important of mutations in isolates from Belarus. In 40 isolates, four types of mutations were identified in codon 315: AGC→ACC ( n = 36)85%, AGC→AGG ( n = 1) 2.3%, AGC→AAC ( n = 2) 4.7%, AGC→GGC ( n = 1) 2.3%. One type of mutation was found in codon 316: GGC→AGC ( n = 18)41.4% and in 15 isolates four types of mutations were detected in codon 309: GGT→GGT ( n = 7)16.1%, GGT→GCT ( n = 4)9.2%, GGT→GTC ( n = 3)6.9%, GGT→GGG ( n = 1)2.7% [Figure - 1]. Two types of mutations were found in codon 357 GAC→CAC and GAC→AAC in two isolates. In addition two mutations which were also observed in codons 463 CGG→CTG and 454 GAG→CGA were found. Nine isolates with one mutation (21.5%), 16 - two mutations (38%), 9 - three mutations (21.5%), four - 4 mutations (9.5%) and 4 - five mutations (9.5%) were also demonstrated in all 42 isolates [Table - 1a & b]. As seen in the figure, silent mutations were detected in codons: 306 (CCG→CCC), 309 (GGT→GGG) and 314 (ACC→ACG) in three isolates. Discussion The majority of hot mutations in katG gene of M. tuberculosis have been reported in codon 315 (Ser →Thr) and less in other codons. [1],[2],[10] Unlike most resistance-conferring mutations, mutations in codon 315 (Ser →Thr) are found to result in near-normal catalase-proxidase activities and virulence along with resistance to isoniazid.. This mechanism of isoniazid resistance is not usually associated with a large reduction in virulence and is an exception to the rule that antibiotic-resistance conferring mutation carry a significant fitness cost. [12] The known genes related to isoniazid-resistance are katG, inhA, ahpC, kasA . [5],[13] Most reports suggest that resistance of M. tuberculosis to isoniazid mostly corresponds to changes in codon 315. [2],[8] Findings of this study were similar with 95% of all isolates showing mutation in codon 315. Our data indicate that highest numbers of mutations observed were 1: 315AGC→ACC (Ser→Thr) 36%, 2: 316 GGC→AGC (Gly→Ser) 14.4%. In this study, 75% of all isolates demonstrated to have mutations in codons 309 ( n = 15, 34%) and 316 ( n = 18, 41.4%) which might represent second most important mutation. Similar results were reported in Latvia in which mutation in codon 315 of katG corresponded to AGC→ACC (Ser→Thr) in 90% cases, however, in our study we have not observed AGC→ACA (Ser→Thr) that was seen in 10% cases of Latvia study. [2] In Poland, 90% of mutations were in codon 315AGC which corresponds to five types of mutations (ACC, ACT, ACA, AAC,ATC) resembling our data on nucleotide ACC and AAC, however we did not observe nucleotide changes on ACT, ACA and ATC. Mutations detected in one strain in codons 463 and 357, 454 and 357, may indicate that this type of mutation in Belarus is less of a concern when compared to neighbouring countries. [5],[6],[9] Other studies have mentioned that silent mutations were never detected in katG gene. [9],[10] However, in this research three silent mutations were obtained which indicated no effect on drug resistant pattern. Four sensitive and one standard strain H37RV were sequenced and used as control and no mutations were detected in these control strains. Authors of this study also believe that sequencing is a good method for determination of mutations among MDR tuberculosis strains compared to spoligotyping and PCR-RFLP. The high percentage of double mutations found among the isolates in Belarus differed clearly from the lower prevalence of double mutations in other studies. A characteristic prominent finding of this study was the high frequency of two (40.47%), three (21.42%), four (9.5%) and five mutations (9.5%) occurring in separate codons [Table - 1a & b]. Of 42 isoniazid resistant isolates, 10 (24%) were isolated from sputum of patients with primary infection. Four of these isolates demonstrated five mutations, four showed four mutations and two isolates showed three mutations, revealing that sputum samples of 10 patients with primary infection demonstrated mutations in codons 315, 316 and 309. Interestingly all single and double mutations were found in isolates taken from sputum samples of patient with secondary infection. Thirty two isolates (76%) of patients with secondary infection (data on reactivation cases not available) were found to have mutations in codon 315(49.2%), 12(19%) in codon 316 and 7(11.1%) in codon 309 [Table - 1a & b]. The highest frequency of common mutation sharing between primary and secondary infections in this study occurred in codon 315. Acknowledgment We thank our colleagues in Belarusian Institutes of Pulmonology and Tuberculosis for sample collection.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08041t1.jpg] [mb08041f1.jpg] [mb08041t1b.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}