 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
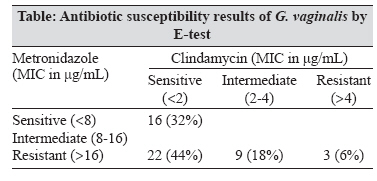
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 155-157 Brief Communication Antibiotic resistance of Gardnerella vaginalis in recurrent bacterial vaginosis Nagaraja P Department of Microbiology, Farwaniya Hospital, Post Box 18373, Kuwait 81004 Date of Submission: 19-Mar-2007 Code Number: mb08044 Abstract Fifty strains of Gardnerella vaginalis isolated from 321 high vaginal swabs over a period of five months were tested for their antibiotic sensitivity. Sixty eight per cent of all isolates were resistant to metronidazole while 76% were sensitive to clindamycin. All the strains isolated from cases with recurrence of infection were resistant to metronidazole. Clindamycin therapy has a better clinical efficacy than metronidazole in cases of recurrent bacterial vaginosis.Keywords: Antibiotic resistance, bacterial vaginosis, Gardnerella vaginalis Bacterial vaginosis (BV) is considered a common vaginal disorder in women of reproductive age. The normal vaginal microflora consists of lactobacilli, especially Lactobacillus crispatus , while the disturbed vaginal microflora is characterised by the overgrowth of Gardnerella vaginalis and other anaerobic bacteria like Mobiluncus spp., Mycoplasma hominis and Prevotella spp. The interest in BV has increased lately because of the evidence on adverse sequelae to this disorder, such as amniotic fluid infection, clinical chorioamnionitis, premature rupture of membranes (PROM), preterm delivery, low birth weight and postpartum endometritis. [1] The odds ratio for PROM has been reported to be 7.3 in women with BV. [2] Non-pregnant women with BV have been reported to get post-abortion pelvic inflammatory disease, [3] post-hysterectomy vaginal cuff cellulitis and plasma cell endometritis. [1] Several publications have also reported an altered vaginal microflora being linked to an increased susceptibility to the acquisition of HIV and other sexually transmitted infectious agents such as Neisseria gonorrhoeae and Chlamydia trachomatis . [4] However, increase in rates of syphilis or Trichomonas vaginalis have not been reported with BV. Treatment regimens for BV use metronidazole or clindamycin, either orally or as vaginal creams. The cure rate with oral therapy after a seven-day course has been 84-96% and 94% respectively for metronidazole and clindamycin. [5] The cure rates with vaginal gels have been reported to be 75% and 86% respectively. [6] Oral therapies with both agents have shown reduced pregnancy-associated morbidity while topical therapies have not. [7],[8] However, both modes of therapy are effective in non-pregnant women. [9] The conventional treatment of BV in our hospital has been the usage of oral metronidazole as per international recommendations. However, in view of an increased frequency of recurrent vaginal discharge in patients treated for bacterial vaginosis, we attempted to detect antibiotic resistance among strains of G. vaginalis as the probable cause. Recurrent infections might be due to the survival of metronidazole or clindamycin resistant bacteria in the vagina. However, it is reported that less than one percent of the cultivable vaginal anaerobic bacteria are resistant to metronidazole. [10] Materials and Methods High vaginal swabs from a total of 321 patients received over a period of five months from June 2006 to November 2006 were chosen for the study. A total of 135 endocervical swabs received from the same group were also processed. Vaginal and endocervical swabs were collected from adults attending the gynaecology outpatient department and clinically diagnosed as bacterial vaginosis, as part of the routine clinical workup of outpatients. Swabs collected from inpatients with a diagnosis of bacterial vaginosis were also included in the study. Separate swabs were collected for the high-vaginal (TRANSWAB, MW170, Medical Wire and Equipment Co. Ltd, Corsham, England) and the endocervical (Collection-Eze, CZ-300 Amies, MML Diagnostics Packaging, Troutdale, OR) specimens in accordance with standard procedures. Direct smear and wet mounts were made to observe for clue cells, pus cells, to grade the smears (Nugent′s criteria) [11] and to observe for Trichomonas vaginalis . The high-vaginal swabs were cultured for gonococci on Thayer Martin Medium (GC Agar Base (CM0367) with 1% Haemoglobin powder (LP0053), Vitox Supplement (SR0090) and VCN Selective Supplement (SR0101E), Oxoid Limited, Basingstoke, England). In addition, the samples were cultured for G. vaginalis on GV Selective medium (CM331 with human blood, 0.02% Tween 80 and GV Selective supplement SR 119), for yeasts on Sabouraud dextrose agar (CM41) and for streptococci on 5% sheep blood agar (CM854) (Oxoid Limited, Basingstoke, England). The inoculated plates (except Sabouraud agar) were incubated for 48 hours at 37°C in 7% CO 2 . Endocervical specimens were processed using a hybridisation assay (Affirm VP III Microbial Identification Test, Becton Dickenson Microbiology Systems, MD) to detect G. vaginalis , Candida spp. and Trichomonas vaginalis . Cultures were interpreted and organisms identified using standard methodologies. [11] Species identification and antibiograms for pathogens were performed using VITEK II (BD Microbiology Systems, MD). Strains of G. vaginalis were tested for antibiotic sensitivity to metronidazole and clindamycin by the E-test (AB Biodisk, Solna, Sweden) in an anaerobic environment using the prescribed methods. Comparative data analysis was carried out using MS Excel 2003. Results A total of 50 strains of G. vaginalis were isolated from the 321 specimens (15.6%). Candida spp. (including C. albicans ) was isolated from 60 of the 321 samples (18.7%). Nine of the 50 samples that yielded G. vaginalis also grew Candida spp., while nine samples grew S. agalactiae and two samples grew both Candida and S. agalactiae all in addition to G. vaginalis . A total of 135 endocervical swabs (ECS) were processed by the Affirm VP III microbial identification kit. Of these, 40 (29.6%) samples were positive for G. vaginalis , seven (5.2%) positive for Candida spp., two (1.5%) for T. vaginalis while eight samples (5.9%) were positive for both G. vaginalis and Candida spp. Overall, 57.8% of the ECS were negative for all the three pathogens. Among the 50 patient samples that grew G. vaginalis , ECS were received in 24 cases for Affirm VP III assay. Of these, 14 (58.3%) were positive for G. vaginalis , Candida in one, T. vaginalis in one, both Candida and G. vaginalis in three (12.3%) and negative in five (20.8%) specimens. Thirty seven (74%) of the 50 G. vaginalis strains obtained were from outpatients while the remaining 13 strains were from inpatients. Among these 50 samples, clue cells were positive in 37 (74%) samples and Nugents criteria demonstrated "bacterial vaginosis" in 42 samples (score 7-10) (84%) and "intermediate" in eight samples (score 4-6). A total of 17 patients (34%) among the 50 cases selected had previous history of similar complaints and therapy with metronidazole and the symptoms had recurred in 4-8 months (Mean of 6 months). Duplicate samples received from the same patient within a two week period were excluded from the study. The antibiotic sensitivity of the 50 strains of G. vaginalis done by E-test is shown in the [Table]. The MIC range for metronidazole was from 0.094 to> 256, while the range for clindamycin was from 0.016 to> 256. Overall, 34 (68%) strains were resistant to metronidazole, while 38 (76%) strains were sensitive to clindamycin. Among the 17 strains of G. vaginalis isolated from patients diagnosed as having recurrent bacterial vaginosis, seven strains were sensitive and 10 strains resistant to metronidazole, while all these isolates were sensitive to clindamycin. Discussion The therapy of bacterial vaginosis (BV) has become a topic of debate with research pointing at the complexity of the issue and probable new pathogens associated with the clinical condition. The primary recommendation for treatment of BV has been metronidazole, (oral or intra-vaginal) given 500 mg twice daily for a week. However, with patients showing recurrence of symptoms within a short period of the completion of the therapy, the causative pathogen and/or its resistance to antibiotics is under focus. Antibiotic resistance is being increasingly reported around the world. Goldstein et al, in 1993 had demonstrated a 20% resistance of G. vaginalis to metronidazole and the same group reported 29% resistance to metronidazole in 2002. [12] We have observed an overall 68% resistance of G. vaginalis strains to metronidazole, a very high rate in the population studied. Recurrence rates of up to 30% within three months after treatment have been reported in literature. [13] This recurrence could be due to the survival of metronidazole or clindamycin resistant bacteria in the vagina. Beigi et al, [10] reported that less than one percent of the cultivable vaginal anaerobic bacteria are resistant to metronidazole. Among the strains we isolated from recurrent BV, 58.8% of the strains were resistant to metronidazole. Since we do not have similar data from the past, a comment cannot be made on the previous level of antibiotic resistance of G. vaginalis in the local population. Other pathogens like Candida and T. vaginalis were also documented in patients investigated with complaints of vaginitis. However, none of the 17 patients who came back with recurrence of symptoms showed either Candida or T. vaginalis . Majority of the patients attend the outpatient clinics and may get lost for follow-up. In our series, 74% of all the G. vaginalis isolates were from the gynaecology outpatients. Patients do return back if they experience a recurrence of symptoms and many a time they approach a different clinic for help. This leads to a loss on follow-up studies. The seven strains of G. vaginalis we isolated from patients with recurrent BV that were sensitive to metronidazole raise issues of other possible causes for the recurrence. A new novel pathogen, Atopobium vaginae is being implicated in BV and has been documented to be metronidazole resistant. [14] However, this elusive pathogen requires molecular methods for detection and the lack of such methods in routine diagnostics poses a hurdle in today′s laboratory medicine practices.The nucleic acid hybridization assay (Affirm VP III Microbial Identification Test, Becton Dickenson Microbiology Systems, MD) is not only rapid but more sensitive and specific than the routine culture technique. Good correlation between this rapid method and the clinical picture has been demonstrated in the past. [11] We were able to diagnose more number of cases of bacterial vaginosis by this method than the cultural techniques. Valuable time can be saved by rapid diagnosis of the incriminating pathogen and instituting prompt therapy. This is also valuable in cases having mixed infections caused by yeasts or parasites, wherein combination therapy is advocated. Clindamycin is now being recommended at 300 mg twice daily for a week in all the cases, instead of metronidazole. Clindamycin, though useful in helping with the remission of BV, is known to affect lactobacilli and thereby the reduction of hydrogen peroxide production, an important factor in preservation of the normal vaginal microflora. [15] However, metronidazole is known not to affect the lactobacilli because of their innate resistance and the rapid recolonisation rate by the H 2 O 2 producing bacilli after a course of the drug. One of the problems with the treatment of BV is that even with sensitive organisms and specific antibacterial agents, the cure rate and reduced recurrence rate for BV is far from optimal. A planned prospective study over an extended period of time would help us evaluate the course of action and to study further the complex issue of recurrent BV and the prevalence of A. vaginae in the local populace. This would also be useful to evaluate the diagnostic and therapeutic protocols in cases of bacterial vaginosis in this part of the world. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08044t1.jpg] |
| |||||||||
{kind=link}