 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 172-175 Brief Communication Chronic diarrhoea in HIV patients: Prevalence of coccidian parasites Gupta S, Narang S, Nunavath V, Singh S Department of Laboratory Medicine, All India Institute of Medical Sciences, New Delhi - 110 029 Date of Submission: 27-Jan-2007 Code Number: mb08049 Abstract The purpose of this study was to determine the prevalence of intestinal parasites in HIV patients with or without diarrhoea and to see an association between diarrhoea and the coccidian parasites in our setting. Stool samples from 113 HIV patients, 34 chronic diarrhoea and 79 without any history of diarrhoea were collected and examined for enteric parasites by microscopy. One hundred and thirteen control samples from HIV negative patients complaining of prolonged diarrhoea were also collected and analysed. Prevalence of coccidian parasites in HIV and non-HIV patients; with and without diarrhoea was compared using chi-square tests. Enteric parasites were detected in 55.8% HIV patients with diarrhoea compared to 16.4% in patients without diarrhoea ( P < 0.001). Isospora belli was found in 41.1% (14/34) of chronic diarrhoea and 6.3% (5/79) in non-diarrhoeal cases ( P < 0.001). Cryptosporidium was detected in 20.6% (7/34) of chronic diarrhoea and 2.5% (2/79) in non-diarrhoeal cases ( P < 0.01). Cyclospora cayetanensis associated diarrhoea was detected in only one case of chronic diarrhoea (2.9%). CD4+ T-cell count was lower (180 cells/μL ) in diarrhoeal HIV patients as compared to non-diarrhoeal patients. Coccidian parasites were seen at a mean CD4+ T-cell count of 186.3 cells/μL. This study concluded that Isospora belli was the predominant parasite followed by Cryptosporidium spp. and both were strongly associated with diarrhoea among HIV patients.Keywords: Human immunodeficiency virus, north-India, opportunistic-enteropathogens India has the distinction of having the largest number of people living with human immunodeficiency virus (HIV) in the world. [1] With an adult prevalence rate of 0.91%, [2] the number of patients presenting with AIDS is also increasing. Despite the widespread HIV awareness programmes going on at the present, a large number of patients either go undiagnosed or present late with multiple infections. Diarrhoea is one of the most common presenting complaints in HIV-infected individuals. The infectious etiological agents include both opportunistic agents that consistently cause severe, chronic or frequent gastrointestinal disease and non-opportunistic agents that usually cause acute, treatable diarrhoeal illness. [3] Chronic diarrhoea, defined as persistence of diarrhoea beyond four weeks [4] is a common symptom in HIV-infected patients in the Tropics. Due to the delayed diagnosis of HIV in these individuals, the patients usually take over-the-counter drugs or local medications for symptomatic relief and the underlying disease is left untreated. In a developing country like India, this often results in weight loss and wasting syndrome leading to profound morbidity. The World Health Organisation (WHO) defines diarrhoea wasting syndrome along with a positive HIV serology test to be an AIDS-defining illness. [5] Yet, diagnosis of HIV in our patients is usually delayed and occurs only when the physician advises for a screening test. Several species of protozoa have been associated with acute and chronic diarrhoea in HIV disease. The most commonly reported include Cryptosporidium parvum , lsospora belli , Microsporidium species, Giardia intestinalis , Entamoeba histolytica and Cyclospora species. Besides these, the nematode Strongyloides stercoralis can cause diarrhoea and overwhelming infestation (hyper infection syndrome) in patients with such immunosuppressive disorders. Only a few studies regarding the prevalence of intestinal parasites and their association with diarrhoea of HIV-infected patients are available from North India at the present. We took up this study at a teaching hospital in North India to evaluate the prevalence of such infections in HIV patients in our set-up and to emphasise the importance of stool examination for the detection of coccidian parasites. Materials and Methods
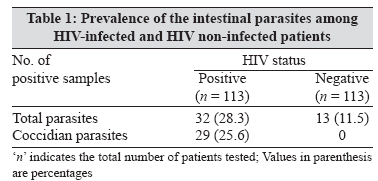
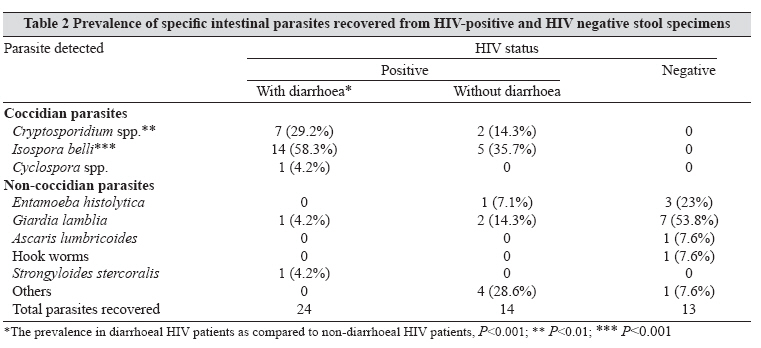
Study design and patient selection Stool examination Statistical methods Results A total of 113 HIV positive patients (250 stool specimens) were examined for the presence of intestinal parasites. Stool samples from 113 HIV negative patients having complaints of persistent or chronic diarrhoea, were also tested during this period.The mean age of the HIV-infected patient group was 33.2 years (range 4-65 years; SD 9.72), with 93 males and 20 females. Chronic diarrhoea was the presenting complaint in 34 patients while 47 presented with undiagnosed fever (PUO), 11 with either pulmonary, extrapulmonary or disseminated tuberculosis, 13 with skin lesions of herpes or other sexually transmitted infections (STIs), two with interstitial pneumonia, three were asymptomatic and three with other non-specific complaints. In the HIV non-infected group, the mean age of the patients was 22.3 years (range 1-65 years, SD 16.9), with 82 males and 31 females. Intestinal parasites were seen in 32 (28.3%) of the 113 samples from HIV-infected individuals whereas only in 13 (11.5%) of the 113 HIV negative samples [Table - 1]. A total of 38 enteric pathogens were detected from HIV samples. Among these, the majority (29) comprised the coccidian parasites detected either alone or in combination with other pathogens. Among the coccidian parasites there was preponderance of Isospora belli (50%) followed by Cryptosporidium spp. (23.6%) and Cyclospora 2.6%. Among the non-coccidian parasites Giardia lamblia (7.8%) was the commonest followed by Strongyloides stercoralis and Entamoeba histolytica (each 2.6%). Among the 13 stool specimens from HIV negative patients, Giardia lamblia (53.8%) was the commonest parasite followed by Entamoeba histolytica (23%), hookworm (7.6%) and Ascaris lumbricoides (7.6%). No opportunistic coccidian parasite was detected from the stool samples belonging to the HIV negative patients [Table - 2]. Among the HIV positive patients, 34 (30.1%) had presented with chronic diarrhoea and the rest 79 patients had other non-diarrhoeal complaints. Intestinal parasites were detected more commonly (55.8%) in patients with chronic diarrhoea than in 16.4% in patients with other complaints ( P < 0.001). In both the patient groups, the coccidian parasites were more common than other protozoa and helminths. The oocysts of opportunistic coccidian parasites (i.e., C. parvum , I. belli and C. cayetanensis ) were also detected more commonly in HIV-infected patients with chronic diarrhoea ( P < 0.001) as compared to the non-diarrhoeal HIV group [Table - 2]. Isospora belli was detected in 14 (41.1%) patients with diarrhoea and five (6.3%) patients without diarrhoea. The association of Isospora belli with diarrhoea among HIV positive individuals was significant ( P < 0.001). Cryptosporidium spp. was detected in seven (20.6%) HIV patients with diarrhoea and two (2.5%) patients without diarrhoea, its association with diarrhoea among HIV patients was also found to be significant ( P < 0.01). Cyclospora was seen only in one (2.9%) HIV patient with diarrhoea and its association with diarrhoea was not found to be significant ( P > 0.05). CD4+ T-cell counts were done in 48 of the 113 patients with HIV. It could not be done in others due to financial constraints. The mean CD4+ T-cell counts were lower in diarrhoeal cases (180 cells/μL) as compared to the non-diarrhoeal cases (261.3 cells/μL). To see a correlation of prevalence of coccidian parasites and CD4+ counts, we calculated the mean CD4+ T-cell counts in these patients and we found that the mean CD4+ counts in patients harbouring coccidian infections (186.3 cells/μL) was lower though not significantly different from patients without coccidian infections (201.4 cells/μL). Discussion Opportunistic infections constitute a major health problem in patients infected with HIV. Among these, intestinal parasitic disease are the commonest and are a major cause of morbidity and mortality in HIV positive individuals worldwide. [6] The coccidian parasites ( Cryptosporidium spp., Isospora belli, Cyclospora spp. and Microsporidium spp.) are foremost among the enteric parasites in these patients. [3] These organisms usually cause a self-limiting illness in immunocompetent individuals but as the immune status of the patient falls they are known to cause life-threatening profuse watery diarrhoea. [7] In the present study enteric parasites were recovered in 30% of HIV patients, with the coccidian parasites comprising 76.3%. Our study shows that Isospora belli (50%) was the most common parasite in HIV positive patients both with and without diarrhoea followed by Cryptosporidium spp. Both I. belli and Cryptosporidium spp. were found to be strongly associated with diarrhoea in HIV patients ( P < 0.001 and P < 0.01 respectively). Earlier studies [8],[9] from North India had found Crytosporidium to be the most common parasite while the prevalence of Isospora belli was found to be much lower. Studies from South India [10],[11] have also reported a higher prevalence of Isospora belli than Cryptosporidium . The present study was also comparable to our previous laboratory data (unpublished) wherein 990 stool samples from 663 HIV positive individuals, both with and without diarrhoea (500 males and 163 females), were tested over five years. A total of 246 enteric parasites were detected in 206 (31.1%) patients with multiple parasites in 29 patients. I.belli (29.2%) was the commonest parasite followed by Cryptosporidium spp. (25.6%), Giardia lamblia (11.8%) and Entamoeba histolytica (5%). The rest included Entamoeba coli (12.6%) and other parasites like Cyclospora spp., Ascaris lumbricoides, hookworm, Blastocystis hominis , Strongyloides stercoralis , Enterobius vermicularis and Hymenolepsis nana , each with a prevalence of 1-2%. Although these opportunistic parasites can be acquired at any time during the course of HIV infection, previous reports suggest that most of the infections with Cryptosporidium are established in patients with CD4+ T-cell counts less than 200 cells/μL . [9],[12] In the present study we also found that diarrhoea in HIV patients was usually associated with low CD4+ T-cell counts (180 cells/μL ). Moreover, the presence of the coccidian parasites was also associated with a lower CD4+ T-cell count in these patients. Multiple infections with Isospora belli and Cryptosporidium spp. were seen in two patients, Isospora belli , Cryptosporidium and Strongyloides stercoralis [13] in one case and Isospora belli and Giardia lamblia in another. All these cases had presented with chronic diarrhoea and a mean CD4+ T-cell counts of 105.3 cells/µL. Due to the easy availability of HAART in developed nations, there has been a reduction in the prevalence of intestinal parasites in AIDS patients. At higher CD4+ T-cell levels, generally, spontaneous clearing of the parasite takes place. In resource poor settings like ours, patients usually go undiagnosed for long periods and present late in the course of the disease. Consequently, the patients usually present with profound, persisting and multiple intestinal infections and a low CD4+ T-cell counts. In a country of 5.2 million HIV positive adults in the 15-49 years age group, India is now faced with multiple concentrated HIV-epidemics. [2] Even though the coccidian parasites are considered AIDS-defining opportunistic pathogens according to CDC, their screening is not done even in known HIV patients in most routine laboratories at the primary care level due to the lack of knowledge, expertise and technique. Therefore, knowledge about the pattern of pathogens can often guide appropriate therapy. In a developing country like India, the magnitude of intestinal parasitic infections in HIV patients further adds to the existing financial burden of the disease. Patients usually belong to poor socio-economic backgrounds and they can hardly afford treatment. Therefore, it is suggested that steps should be taken to prevent the occurrence of these diseases in AIDS patients, as often the disease may take a fulminant form. This can be done by drinking safe water and avoiding contact with contaminated soil. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08049t2.jpg] [mb08049t1.jpg] |
| |||||||||
{kind=link}
{kind=link}